Article Text

Abstract
Objective The primary objective was to assess the performance of a new generation thin-strut sirolimus-eluting coronary stent with abluminal biodegradable polymer in an all comer population. The secondary objective was to detail differences in contemporary percutaneous coronary intervention (PCI) practice worldwide.
Methods e-Ultimaster was an all-comer, prospective, global registry (NCT02188355) with independent event adjudication enrolling patients undergoing PCI with the study stent. The primary outcome measure was target lesion failure (TLF) at 1 year, defined as the composite of cardiac death, target vessel myocardial infarction and clinically driven target lesion revascularisation. Data were stratified according to 4 geographical regions.
Results A total of 37 198 patients were enrolled (Europe 69.2%, Asia 17.8%, Africa/Middle East 6.6% and South America/Mexico 6.5%) and 1-year follow-up was available for 35 389 patients (95.1%). One-year TLF occurred in 3.2% of the patients, ranging from 2% (Africa/Middle East) to 4.1% (South America/Mexico). In patients with acute coronary syndrome, potent P2Y12 inhibitors were prescribed in 48% of patients at discharge, while at 1 year 72% were on any dual antiplatelet therapy. Lipid-lowering treatment was administered in 80.9% and 75.5% of patients at discharge and 1 year, respectively. Regional differences in the profile of the treated patients as well as in PCI practice were reported.
Conclusions In this investigation with worldwide representation, contemporary PCI using a new generation thin-strut sirolimus-eluting coronary stent with abluminal biodegradable polymer was associated with low 1-year TLF across clinical presentations and continents. Suboptimal adherence to current recommendations around antiplatelet and lipid lowering treatments was detected.
- coronary artery disease
- percutaneous coronary intervention
Data availability statement
Data are available on reasonable request. Data also uploaded as online supplemental material.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Percutaneous coronary intervention (PCI) is the the most common modality of coronary revascularisation and among the most frequently performed therapeutic procedures in medicine.1 While PCI has been extensively studied in large-scale national registries2–4 as well as in randomised controlled trials comparing it with medical management or coronary artery bypass surgery,5–7 comparative data on contemporary PCI practice across the globe are lacking. The main purpose of the e-Ultimaster registry was to assess the performance of a new generation thin-strut sirolimus-eluting coronary stent with abluminal biodegradable polymer in an all-comer patient population worldwide to complement the favourable data generated in randomised controlled trials.8 9 A secondary objective of this analysis was to describe contemporary PCI practice worldwide.
Methods
Study design
The e-Ultimaster registry (NCT02188355) was an all-comer, single-arm, prospective, multicentre study, with clinical follow-up at 3 months and 1 year, evaluating the performance of a new generation thin-strut sirolimus-eluting coronary stent with abluminal biodegradable polymer (Ultimaster; Terumo Corporation, Tokyo, Japan) in daily practice. Patients were enrolled between October 2014 and June 2018 in 378 hospitals from 50 countries (online supplemental table 1). Follow-up was performed at 3 months at 1 year, by phone or hospital visit. Information collected included vital status, occurrence of adverse events, angina status, antiplatelet medication and other cardiac medication. Sites were instructed to attempt three phone calls and one contact by letter to obtain follow-up information before patient was considered lost to follow-up. For the purpose of the analysis, countries were grouped in four geographical regions: Europe, Asia, South America/Mexico and Africa/Middle East (online supplemental figure 1 and online supplemental table 2). No patient or public was involved in the design or execution of the study.
Supplemental material
Study population and device
All patients ≥18 years old undergoing PCI using a drug-eluting stent according to local hospital practice and with the intention to be implanted with the study stent were eligible. The registry was conducted in accordance with the Declaration of Helsinki and country-specific regulatory requirements. The study protocol was reviewed and approved by the Institutional Review Board/Ethics Committee of each participating centre and all patients signed the informed consent form. The study population used to analyse clinical outcomes during follow-up includes all patients who received one or more study stents on enrolment and (1) completed 1 year follow-up or (2) who reached the primary outcome measure or (3) who died during follow-up. The Ultimaster coronary stent system is a new generation open-cell cobalt–chromium thin-strut (80 µm) sirolimus-eluting stent with an abluminal biodegradable polymer coating (poly-D,L-lactic acid polycaprolactone).10 Sirolimus is released over a 3-month to 4-month period after which the polymer coating is fully degraded.
Clinical outcomes
The primary outcome measure was target lesion failure (TLF) at 1 year, defined as a composite of cardiac death, target vessel myocardial infarction and clinically driven target lesion revascularisation (endpoint definitions reported in online supplemental table 3). Prespecified secondary outcome measures included any death, cardiac death, myocardial infarction, target lesion revascularisation, target vessel revascularisation, target vessel failure (composite of cardiac death, target vessel myocardial infarction and target vessel revascularisation), the composite of any death, any myocardial infarction and any coronary revascularisation, stent thrombosis, and major vascular and bleeding complications. A clinical events committee reviewed and adjudicated all the reported adverse events possibly related to death, myocardial infarction, target lesion or target vessel revascularisation and stent thrombosis (online supplemental table 4). For the purpose of the study, length of stay was defined as [(date of discharge–date of procedure)+1]; that is, length of stay=1 means discharge on the same day of the procedure.
Statistical analysis
Patient demographics, comorbidities, target lesion characteristics, procedural characteristics and medication use were analysed per geographical region and were summarised using mean±SD for continuous variables and frequencies and percentages for categorical variables. A comparison was made over all regions, using ANOVA (if variances were equal) or Welch test (if variances were unequal) for continuous variables and χ² test for categorical variables. In addition, comparisons were made between each region and Europe, using Student’s t-test (parametric) or Kruskal-Wallis test (non-parametric) for continuous variables and χ² test or Fisher exact test for categorical variables. A univariate logistic regression model was used to calculate the OR with 95% CI for primary and secondary outcome measures for each region as compared with Europe. To identify predictors of the primary outcome measure, a stepwise logistic regression model was used with p values to enter and stay in the model set to p=0.25 and p=0.10, respectively. The variables entered in the model were age, sex, body mass index, diabetes mellitus, hypertension, hypercholesterolemia, smoking, renal failure, previous PCI, previous coronary artery bypass surgery, previous myocardial infarction, non-ST-elevation acute coronary syndromes (NSTE-ACS), ST-elevation myocardial infarction (STEMI), multivessel disease, number of lesion identified, number of lesions treated, treated vessel, bifurcation, chronic total occlusion, in-stent restenosis, ostial lesions, moderate to severe calcification, AHA/ACC lesion type, small vessels, long lesions, number of implanted study stents, length of implanted study stent, radial access and geographical region. Missing values were imputed with the mean value of the selected group. Statistical analyses were performed using SAS software, V.9.4 (SAS Institute, Inc., Cary, NC, USA).
Results
Patient and procedural characteristics
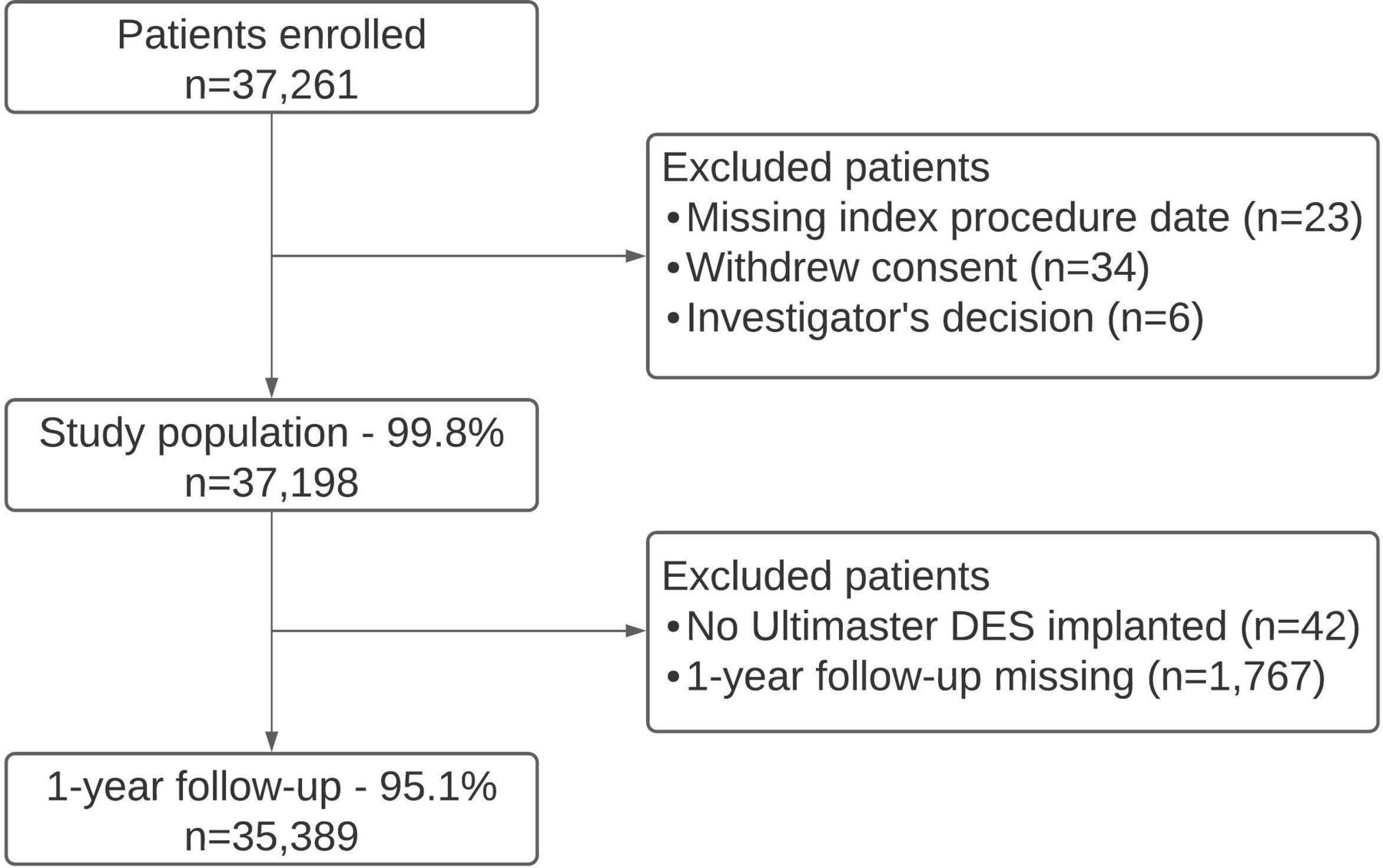
A total of 37 198 patients were included in the study and 35 389 patients (95.1%) completed 1-year follow-up (figure 1). With respect to regional distribution, 25 736 (69.2%), 6614 (17.8%), 2438 (6.6%) and 2410 (6.5%) patients were enrolled in Europe, Asia, Africa/Middle East and South America/Mexico, respectively. Patient’s characteristics stratified per region of enrolment are summarised are detailed in table 1. The majority of the patients across the continents were treated for ACS, while STEMI patients comprised 20.2% of the overall cohort. Details on coronary artery disease at angiography and on the characteristics of the lesions treated are reported in table 2.
Baseline patient characteristics
Coronary artery disease at angiography and characteristics of the treated lesions
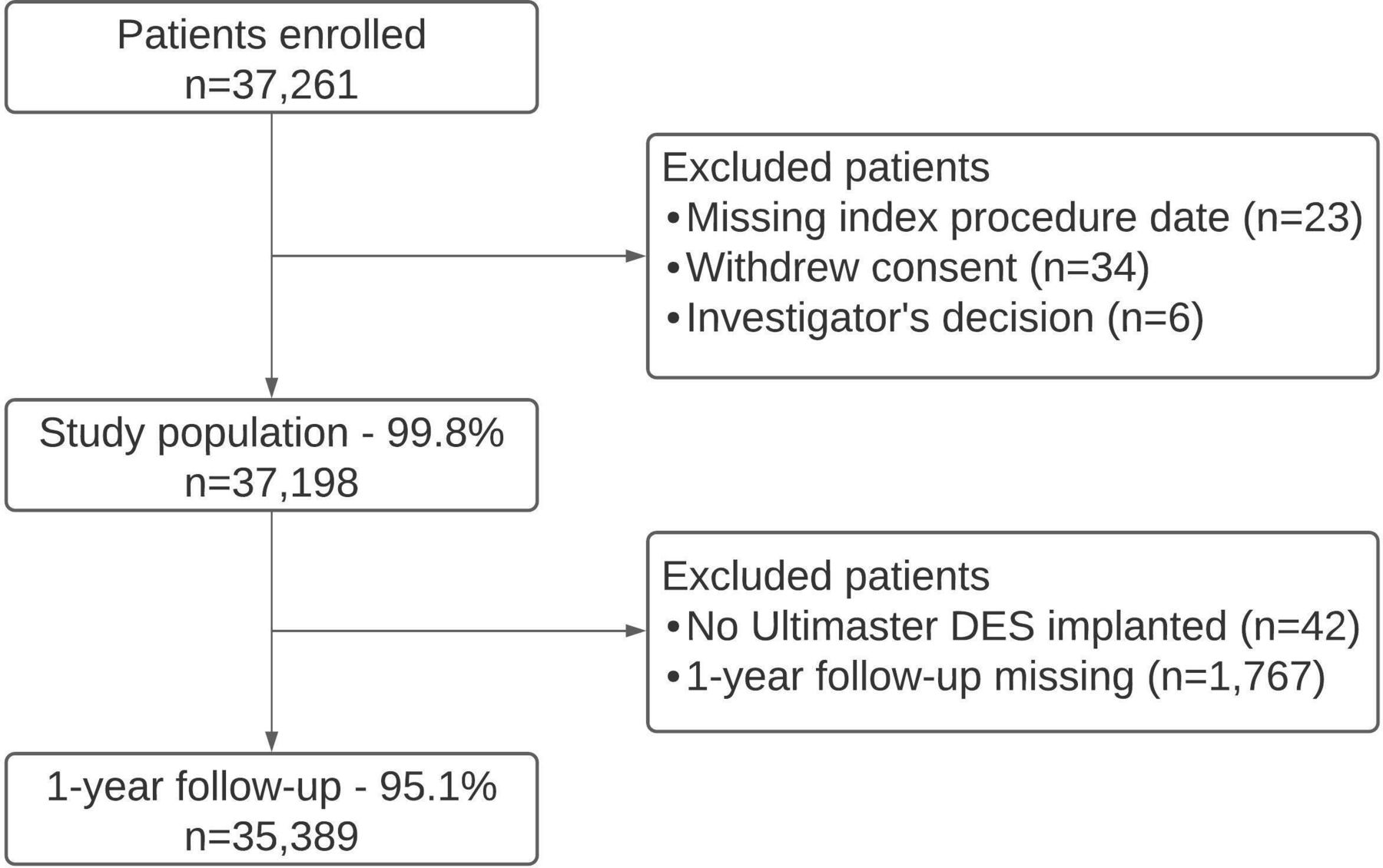
Flow chart of the study population. The 1-year follow-up population included patients who had event that contributed to the primary outcome measure, died during follow-up or completed 1-year follow-up. DES, drug-eluting stent.
The proportion of patients undergoing PCI via transradial access ranged from 50.2% (Africa/Middle East) to 88.1% (Europe). This access route was used in 80.1% of patients with chronic coronary syndromes (CCS), 84.3% of patients with NSTE-ACS and 83.5% of patients with STEMI (p<0.001) (figure 2). Technical details on the PCI procedure are reported in online supplemental table 5. In the vast majority of cases, the procedure consisted of solely balloon angioplasty and stenting, while the use of additional devices such as atherectomy or cutting balloons was limited to 1.1% or less of the procedures in all continents. Balloon dilatation prior to stent deployment (ie, pre-dilatation) was performed in 51.4% (Africa/Middle East) to 59.3% of lesions (South America/Mexico), while balloon post-dilatation to optimise stent expansion was applied in 37.4% (South America/Mexico) to 47.5% (Asia) of lesions. In STEMI, thrombus aspiration was performed in 9.4% (Africa/Middle East) to 21% of the patients (Asia), while in saphenous vein graft interventions, distal protection was applied in 5.4% of cases. Intravascular imaging was rarely used, with the exception of Japan (97.5% use) (online supplemental figure 2). The use of closure devices for femoral access ranged from 9.6% (Asia) to 72.6% (Europe).

Radial access according to clinical presentation per region. CCS, chronic coronary syndrome; NSTE-ACS, non-ST-segment elevation acute coronary syndrome; STEMI, ST-segment elevation myocardial infarction.
Antithrombotic and lipid-lowering treatments
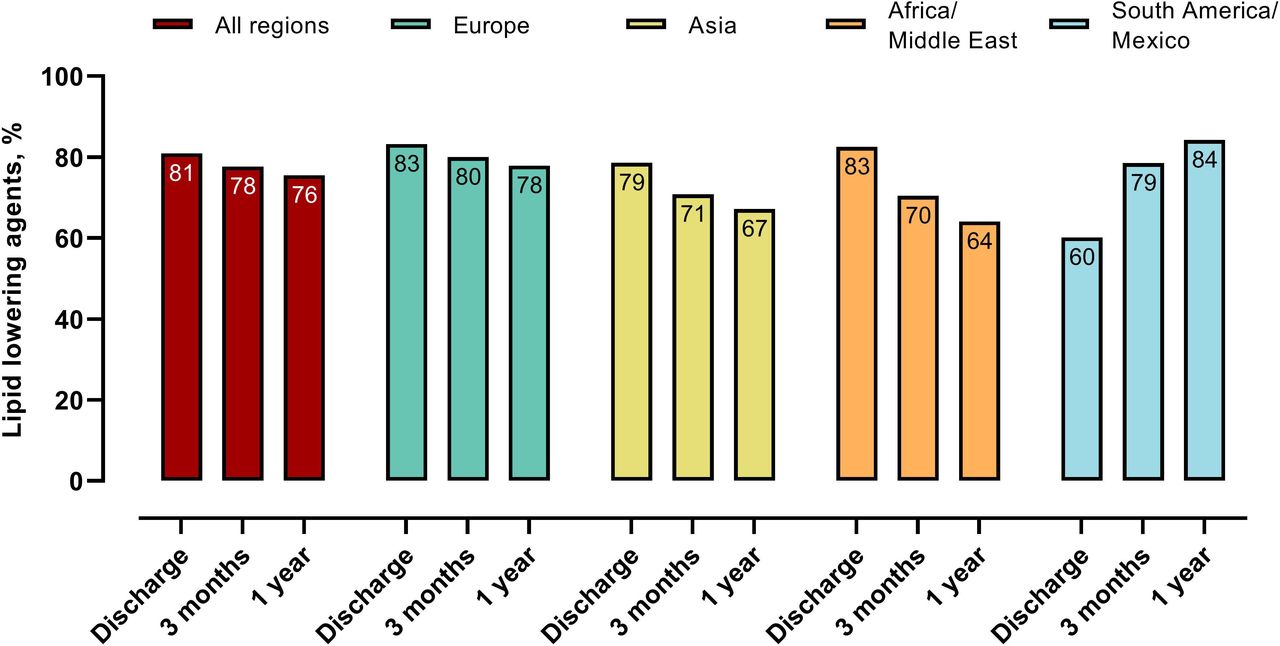
The use of unfractionated heparin during PCI exceeded 90% across the continents, with the exception of Asia, where low molecular weight heparin was used in 31% of the cases (in 11% in patients with CCS and in 46% in patients with ACS) (online supplemental table 6). Intravenous glycoprotein IIb/IIIa receptor inhibitors were used in less than 2% and 10% of PCI for CCS and ACS, respectively. The use of dual antiplatelet therapy (DAPT) at discharge, 3 months and 1 year stratified for the clinical presentation across the continents are depicted in figure 3 and online supplemental table 7. Potent P2Y12 inhibitors at discharge were administered in 48.0% of patients with ACS (online supplemental table 7 and online supplemental figure 3). A total of 6.1% of patients were discharged on oral anticoagulants, ranging from 2.0% (South America/Mexico) to 7.5% (Europe). Prescription of lipid-lowering therapy (ie, of any lipid-lowering agent) in the overall population was 80.9% at discharge and 75.5% at 1 year (figure 4). Rates of lipid-lowering agents at 1 year according to region and clinical presentation are reported in online supplemental table 8.

Dual antiplatelet therapy at discharge and at follow-up according to clinical indication. ACS, acute coronary syndrome; CCS, chronic coronary syndrome; DAPT, dual antiplatelet therapy.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Lipid-lowering treatment in the overall patient population.
Periprocedural complications, length of stay and 1-year clinical outcomes
Angiographic complications, defined as coronary perforation or spasm, no reflow, side branch occlusions or residual thrombus, occurred in 2.3%, 3.1% and 5.2% in patients presenting with CCS, NSTE-ACS and STEMI, respectively (p<0.0001). Online supplemental table 9 reports the event rates stratified per clinical presentation and geographical region. The median (10th−90th percentile) length of hospital stay post-procedure ranged from 2 (1−4) for patients with CCS to 3 (1–7) for NSTE-ACS, and 4 (2–10) for patients with STEMI. Regional data for length of hospital stay post-procedure are reported in online supplemental table 10. The primary outcome measure of the study, TLF at 1 year, occurred in 3.2% of the patients, while definite or probable stent thrombosis and bleedings at 1 year occurred in 0.7% and 2.9% of the patients, respectively. Table 3 summarises the 1-year clinical outcomes stratified per region while the corresponding event rates according to clinical presentations are reported in online supplemental tables 11−13. Independent predictors of TLF at 1 year are reported in table 4.
One-year clinical outcomes
Predictors for 1-year target lesion failure
Discussion
The main finding of e-Ultimaster, a global registry with independent event adjudication, was that PCI performed with a new generation thin-strut sirolimus-eluting coronary stent with abluminal biodegradable polymer was associated with low rates of TLF at 1 year across patient’s clinical presentations and continents (<5% for virtually all analyses). Device safety was remarkable with a definite or probable stent thrombosis rate at 1 year <1%. These results expand to an all comer and far bigger population treated in clinical practice the favourable outcomes of PCI with the same device observed in randomised controlled trials, which have previously shown a 1-year TLF rate of 5.4% among 551 patients with stable and unstable coronary disease and a 1-year TLF rate of 6.1% among 375 patientgs with STEMI.9 11 Independent predictors of 1-year TLF in our study included clinical characteristics such as age, diabetes, renal insufficiency, ACS at presentation and previous revascularisation as well as lesion-specific and procedural predictors, all markers of disease complexity. The performance of PCI in Europe, as compared with Asia and Africa/Middle East, was associated with an increased risk of TLF. The observational nature of the study does not allow conclusion on whether this finding may be due to differences in technique, case selection or unmeasured confounders.
The true global nature of the study allowed for an unprecedented simultaneous assessment of current PCI practices across different regions in the world. Accordingly, worldwide comparative data on contemporary PCI practices are lacking while available data are limited to few countries and specific aspects of the procedure, such as antiplatelet treatment or vascular access.12 13 Limitations of the few ‘global’ PCI studies included the use of first-generation drug-eluting stents or an enrolment essentially limited to Western countries.14 15 We detected major differences in the profile of patients undergoing PCI, procedural practices, pharmacological treatments and outcomes. With respect to the profile of the patients treated, the majority were men over the age of 60 years, while the proportion of octogenarians differed by more than a factor 2 across the continents. More than a quarter of the patients had diabetes, with the prevalence approaching half in Africa/Middle East. In accordance to current guidelines, the main indication for PCI across the continents was ACS.16–18 Our study showed that radial access has become the vascular access site of choice worldwide, with a use ranging from one out of two procedures in Africa/Middle East to virtually nine out of ten in Europe. While in Europe the use of radial approach was widely embraced for all clinical presentation, in Asia and Africa/Middle East this access route was more frequently used in patients with ACS than those with CCS. The choice of the transradial approach for the entire spectrum of clinical presentations is in line with recent guidelines and supported by our study, showing that the use of this vascular access site was protective with respect to 1-year TLF.19 For patients treated via a femoral approach, the use of vascular closure devices showed a great deal of variation, ranging from less than 10% in Asia to almost three-quarters of all cases in Europe. In the absence of adequately powered randomised controlled trials, current guidelines do not provide recommendations in favour or against the use of those devices.
In our study, the PCI procedure consisted of solely balloon angioplasty and stenting in the vast majority of cases, while additional devices such as atherectomy or cutting balloons were rarely used (in 2% or less across the continents). We showed that balloon dilatation prior to stent implantation was more frequently performed than balloon post-dilatation (applied in less than half of the cases). Intravascular imaging was rarely performed, with the exception of Japan where it was used in the vast majority of procedures. The old and inexpensive unfractionated heparin remained the peri-procedural anticoagulant of choice across patient’s clinical presentations and continents, being used in more than 9 out of 10 procedures.18 19 Glycoprotein IIb/IIIa receptor inhibitors were rarely administered, even in the setting of ACS. Virtually all patients received DAPT at discharge. However, approximately 1 out of 5 of patients presenting with CCS was discharged on ticagrelor or prasugrel instead of the guideline-recommended clopidogrel. In addition, DAPT was still administered in 2 out of 3 patients with CCS at 1 year, while the recommended DAPT duration for this indication is 6 months.20 The proportion of patients with CCS on DAPT at 1 year was as high as 8 to 9 out of 10 patients in Asia, Africa/Middle East and South America/Mexico, although such a strategy has been associated with increased bleeding risk in the absence of an ischaemic benefit.21 Remarkable was the finding that less than half of patients with ACS were discharged on a potent P2Y12 inhibitor (ie, ticagrelor or prasugrel), with a proportion being as low as 1 in 7 in South America/Mexico. This was despite the strong recommendation in guidelines for both agents over clopidogrel.18 Likely explanation for this finding is that in some countries these agents may either not be commercialised or too expensive. In all regions, the prescription of ticagrelor surpassed by more than a factor 6 the one of prasugrel. The guideline-recommended DAPT duration of 1 year in ACS was prescribed in less than three quarters of the patients, with Europe showing the lowest rate (2 out of 3 patients), while in other continents the rate exceeded 80%.18 Although e-Ultimaster did not collect all the parameters allowing for a formal bleeding risk assessment, the risk profile of the patients (eg, mean age 64 years, renal insufficiency 7%, prior stroke 5%, need for oral anticoagulation 6%) and the low bleeding rates observed do not seem to justify earlier DAPT discontinuation. Our findings are in line with an international myocardial infarction registry showing that 1 patient out of 4 was not on DAPT at 1 year.13
Despite the wealth of data and the clear-cut recommendations for secondary prevention for lipid-lowering agents, our study demonstrates that lipid-lowering treatment was suboptimal, with approximately 1 in 5 and 1 in 4 patients not receiving lipid-lowering treatment at discharge and 1 year, respectively.22 Our findings reproduce on a global scale prior observation from national and multi-national registries.23 Little is known about differences in current length of stay following PCI across the globe. In our study, the post-procedural length of stay ranged considerably according to clinical presentation and geographical areas. The greatest variation was observed in the rate of same-day discharge among patients treated with PCI for CCS, ranging from 1/20 in Asia to 2/3 in South America/Mexico. Such differences cannot be explained by medical reasons alone and are likely related to specificities of the healthcare system and reimbursement issues. Notable was the variation in post-procedural length of stay we observed in patients with STEMI, ranging from a median of 4 days in Europe and Africa/Middle East to a median of 6 days in Asia.
Our study has several limitations inherent to the nature of the investigation. While the registry had no exclusion criteria other than age less than 18 years and unwillingness to sign the informed consent and encouraged the enrolment of a true all-comer population, the 1-year mortality observed is substantially lower than the one documented in other PCI datasets with systematic inclusion, revealing the selection of a low-risk population.24 25 While all deaths, myocardial infarctions, target lesion and target vessel revascularisations as well as stent thromboses were adjudicated by an independent clinical events committee, other outcome measures were not. Since the measurement of cardiac enzymes post-PCI was left at the discretion of the investigators according to local practice, the incidence of periprocedural myocardial infarctions may have been underestimated. While systematic online data monitoring was performed, underreporting of events cannot be excluded. Enrolment was not equally distributed among regions; however, even in regions less well represented, such as Africa/Middle East and South America/Mexico, the recruitment approached 2500 patients. In addition, practice in countries aggregated to a region were likely non-homogenous. As the study stent was not overall approved, countries with high PCI volumes such as the USA or China could not be included in the study. Finally, loss to follow-up (less than 5%) may have been a source of bias. Baseline characteristics of patients with and without follow-up are reported in online supplemental table 14.
In summary, this study, unmatched to our knowledge in size as well as global representation, showed a remarkable performance of a new generation thin-strut biodegradable-polymer sirolimus-eluting stent, with low TLF as well as stent thrombosis rates at 1 year across clinical presentations and continents. Differences in PCI practice across the globe, such as in the use of transradial access, were outlined and suboptimal adherence to current recommendations on DAPT as well as lipid-lowering therapies were detected. Notable was the administration of DAPT 1 year post-PCI in the vast majority of patients with CCS in several regions of the world and the low prescription rate of potent P2Y12 in patients with ACS. These findings are a call for standardisation of PCI practice and pharmacological treatment post-PCI. Tools to facilitate worldwide implementation of guideline-recommended treatments should be investigated.
Key messages
What is already known on this subject?
While randomised controlled trials have established the efficacy and safety of a new generation thin-strut sirolimus-eluting coronary stent with abluminal biodegradable polymer, information on the performance of the device in a real-world setting are sparse. Although percutaneous coronary intervention (PCI) is one of the most frequently performed invasive therapeutic procedures in medicine, data on contemporary practice worldwide as well as on regional differences are lacking.
What might this study add?
This study expands the favourable performance profile of the study stent observed in randomised controlled trials to an all-comer population in daily practice. In addition, it outlines differences in PCI practice worldwide and showed, among other findings, a suboptimal prescription of antiplatelet as well as lipid-lowering agents.
How might this impact on clinical practice?
This study supports the use of a new generation thin-strut sirolimus-eluting coronary stent with abluminal biodegradable polymer, independently of clinical presentation and local PCI practice. In addition, it calls for a better compliance with practice guidelines, in particular with respect to pharmacological treatment post-PCI.
Data availability statement
Data are available on reasonable request. Data also uploaded as online supplemental material.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. The study protocol was reviewed and approved by the Institutional Review Board/Ethics Committee of each participating centre (378 hospitals from 50 countries). A complete list with all reference numbers/ID can be obtained on request, Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @MMamas1973
Correction notice This article has been corrected since it was first published. Author name 'Shoichi Kuramitsu' has been corrected and the e-ULTIMASTER investigators have been added to the author list.
Collaborators e-ULTIMASTER investigators: Oscar Mendiz, Juan Manuel Telayna, José Magni, Fernando Cura, Juan Lloberas, Mikayel Adamyan, Davit Minasyan, Shahen Khachatryan, Boghos Sarkissian, Hamayak Sisakian, Clemens Steinwender, Irene Lang, Gabor Toth-Mayor, Fazila Tun-Nesa Malik, Alexander Beimanov, Oleg Polonetsky, Jan Nimmegeers, Suzanne Pourbaix, Stéphane Carlier, Adel Aminian, Antoine Guédès, Philippe Decroly, Willem De Wilde, Dries De Cock, Bernard De Bruyne, Joelle Kefer, Maria Sanali Paiva, Bruno Palmieri Bernardi, Jamil Abdalla Saad, Marco Vugman Waistein, Gustavo De Moraes Ramalho, Roberto Otsubo, Rogério Tumelero, Alexandre Tognon, Marcos Franchetti, João Eduardo Tinoco De Paula, Bruno Cupertino Migueletto, Sevdalin Topalov, Krasimir Pandev, Dimitar Karageorgiev, Diana Trendafilova-Lazaroba, Angel Mitov, Borislov Borisov, Dobrin Vassilev, Julia Jorgova-Makedonska, Carlos Romero, Pablo Pedreros, Gabriel Maluenda, Luis Perez, Bernhard Westerberg, Victor David Assef, Angel Puentes, Hugo Castaño, Tamara Gorgadze, Boris Eduardo Vesga, Hector Hernandez, Ladislav Groch, Miroslav Erbrt, Alexandr Schee, Viktor KočKa, Zdenek Coufal, Hany Ragy, Yasser Sadek, Mohamed Abdel Aziz, Hussien Heshmat, Mounir Asman, Ihab Daoud, Ahmed Emara, Hisham Ammar, Mohamed Helal, Tarek Rashid, Mohamed Setiha, Sameh Ahmed Salama, Hazem Khamis, Peep Laanmets, Jean-Louis Leymarie, Emmanuelle Filippi, Simon Elhadad, Chaib Aures, Fabien De Poli, Charlotte Trouillet, Jean-Louis Bonnet, Grégoire Rangé, Nicolas Delarche, Francois Funck, Olivier Dubreuil, Pascal Goube, Stanislas Champin, Pierre Henon, Florent Chevalier, Denis Amer Zabalawi, Emmanuel Boiffard, Thierry Joseph, Olivier Bizeau, Alain Furber, Farzin Beygui, Pascal Motreff, Sebastien Levesque, Julien Rosencher, Pradip Kumar Sewoke, Christophe Piot, Laurent Delorme, Michael Angioi, Max Amor, Gilles Bayet, Yves Biron, Matthieu Godin, Julien Jeanneteau, Jean Luc Banos, Romain Cador, Jacques Monsegu, Stéphane Champagne, Plastaras Philoktimon, Hakim Benamer, Philippe Brunel, Bernard Chevalier, Thomas Hovasse, Fabrice Leroy, Guillaume Lecoq, Levy Raphy, Bernard Karsenty, Alexandre Avran, Ashok Tirouvanziam, Olivier Morel, Pascal Barraud, Philippe Commeau, Lasha Chantladze, Jambrik Zoltan,Lajos Nagy,Andras Vorobcsuk,Ivan Horvath,Bela Merkely,Kôszegi Zsolt,Ingibjörg Jóna Guðmundsdóttir, Gurpreet Singh Wander, R. Keshava, Rajpal Abhaichand, Anil Potdar, Prakash Chandwani, Ajit Bhagwat, Rajendra Kumar Premchand, Ajit Mullasari, B B Chanana, Viveka Kumar, Praveen Chandra, Ashwani Mehta, Bijulal Sasidharan, Prashant Jagtap, Bambang Budiono, Muhammad Munawar, Muhammad Yamin,Yudi Her Oktaviono, Abdul Hakim Alkatiri,Teguh Santoso, Doni Firman, Sasmojo Widito, Eugene McFadden, Jim Crowley, Thomas Kiernan, Minha Saar, Marc Brezins, Ariel Roguin, Majdi Halabi, Ren Kawaguchi, Satoru Otsuji, Yoshito Yamamoto, Makoto Kadotani, Takayuki Ishihara, Kenji Ando, Shoichi Kuramitsu, Katsuhiro Kawaguchi, Yasunori Nishida, Hideo Nishikawa, Shozo Ishihara, Yasuhiro Tarutani, Takashi Morita, Masami Nishino, Keiji Hirooka, Shiro Ono, Yoshiaki Ito, Makoto Muto, Kenshi Fujii, Seiji Yamazaki, Hisayuki Okada, Kazuhiro Ashida, Shigeru Saito, Hiroshi Suzuki, Takashi Matsukage, Imad Alhaddad, Maxat Kudratullayev, Marat Alikhanov, Vadim Seisembekov, Marat Aripov, Dauren Teleuov, Bauyrzhan Ormanov, Ruslan Baisebenov, Azamat Kenzhinovich Zhashkeyev, Azamat Yerzhanov, Orazbek Sakhov, Ersin Sabitov, Vladimir Kotevski, Daou Abdo, Ahmad Serhal, Ramunas Unikas, Aurimas Knokneris, Vladimir Ristovski, Sasko Kedev, Chong Yoon Sin, Abdul Kahar Ghapar, Abd Syukur Bin Abdullah, Siti Khairani bt Zainal Abidin, Tee Chee Hian, Nicholas Chua Yul Chye, Santiago Sandoval Navarrete, Juan Jorge Beltran Ochoa, Sergio Alonso Villareal Umaña, Carlos Ramon Rodas Caceres, Rhizlan Cherradi, Anass Assaidi, Dounia Benzaroual, Fahd Chaara, Martijn Scholte, Alexander J.J. Ijsselmuiden, W.A.L. Pim Tonino, Jawed Polad, Jacob van Eck, Pieter Cornelis Smits, Fabrizio Spano, Lucas H. Savalle, Clemens Von Birgelen, Peter W. Danse, Gillian Jessurun, Pieter Bisschops, Amr Hassan, Adam Witkowski, Adrian Wlodarczak, Maciej Lesiak, Pedro Canas Da Silva, Alexandru Voican, Mihai Ursu, Milovan Slovenski, Ioan Bitea Cornel, Samih Lawand,Tarek Kashour, Muhammad Aurangzaib Mughal, Dragan Sagic, Nikola Jagic, Vladan Vukcevic, Alexandar Davidovic, Sasa Hinic, Martin Hudec, Shiraz Gafoor, Ismail Soosiwala, Graham Cassel, Martin Tawanda Butau, Jean-Paul Theron, Jean Vorster, Pieter Blomerus, Iftikar Osman Ebrahim, Jacobus Badenhorst, Joan Antonio Gomez, Nicolás Vázquez Gonzalez, Fernando Sarnago, Iñigo Lozano, José Ramón Ruiz Arroyo, Ramiro Trillo Nouche, Juan Sanchís, Juan Alcibar, Mariano Larman, José Ramón Rumoroso, José Suárez de Lezo, Maria López Benito, Pablo Cerrato Garcia, Baltasar Lainez, Beatriz Vaquerizo, Javier Botas, Eduard Fernández Nofrerias, Pascual Baello Monge, Fernando Lozano Ruiz-Poveda, Jesus Maria Jimenez Mazuecos, Javier Robles, José Ramon Lopez Minguez, Pepi Garcia, Jorge Palazuelos, Gema Miñana, Jose Javier Zueco, Andrés Iñiguez Romo, Eulogio Garcia Fernandez, Javier Goicolea, Manuel Pan,Arturo García Touchard, Javier Fernández, Javier Fernandez Portales, Gonzalo Peña, Antonio Peñaranda Serra, José Domingo Cascón, Alfonso Torres, Pedro Martin Lorenzo, Javier Balaguer Requena,Raymundo Ocaranza Sanchez, Jose Antonio Diarte de Miguel, Bruno García Del Blanco, Eduardo Pinar, P. José Moreu Burgos, Juan Manuel Duran, Ramón López Palop, César Moris-De La Tassa, Robert Kastberg, Finn Hjortevang, Jason Stewart, Espen Haugen, Ole Fröbert, Peter Wenaweser, Edoardo De Benedetti, Maro Roffi, Gregor Leibundgut, Michael Neuhaus, Florim Cuculi, Wirash Kehasukcharoen, Arthit Wongsoasup, Niphonth Srisuwanunt, Mohamed Akram Drissa, Ben Chedli Tarek, Sami Bouziri, Elyes Kharrat, Mohamed Najeh Abid, Saloua Trabelsi, Rridha Ennouri, Andriy Khohlov, Sergii Salo, Yevhenii Aksonov, Georgiy Mankovskiy, Mohammad Andron, Arif Al Nooryani, Syed Nazir, Muhammad Adnan Raufi, Albert Alahmar, Hesham Ahmed Osman, Seyed Bagher Tabatabaei, Khaled Galal, Murali Krishna, Fahad Omar Baslaib, Rohan Jagathesan, Ramesh de Silva, Jonas Eichhofer, John Kurian, Sanjay Kumar, Javed Iqbal, David Walker, Rajiv Das, Piers Clifford, David Austin, Javed Ehtisham, Ifti Fazal, Kelvin Lee, Paul Kotwinski, Shahzad Munir, Alisdair Ryding, Ahmed Elghamaz, Girish Viswanathan, Sagar Doshi, Sachin Jadhav, Nicos Spyrou, John Mcdonald, Suneel Talwar, Robert Smith, Sen Devadathan, Kamal Chitkara, Sundeep Kalra, James Cullen, Mamas Mamas, David Hildick-Smith, Kevin Carson, Tim Wells, Chetan Varma, James Richardson, Clive Lawson, Rajathurai Thirumaran, Hussain Contractor, Rito Mitra, Ian Hudson, Sukhinder Nijjer, Nicholas Pegge, Helen Routledge, V J Karthikeyan, Mirjamol Mirumarovich Zufarov, Nguyen Van Tan.
Contributors MR is responsible for the overall content as the guarantor. MC interpreted the results and drafted the manuscript. MR participated in data collection, interpreted the results and drafted the manuscript. LJ and RD extracted the data and performed the statistical analyses. All other authors participated in data collection and provided a critical review of the manuscript.
Funding the e-Ultimaster registry was sponsored by Terumo. Terumo is the manufacturer of the Ultimaster stent.
Competing interests The following authors declare a competing interest with Terumo, the sponsor of the study: JP declared consulting fees; MM declared consulting fees and research grants; AA declared consulting fees; MA declared consulting fees; SK declared consulting fees; DJRH-S declared speaking fees and research grants; MR declared research grants. LJ and RD are employees of Terumo. All other authors have nothing to disclose.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.