Abstract
Background: Caffeine intake from one cup of coffee one hour before adenosine stress tests, corresponding to serum caffeine levels of 3-4 mg/L, is thought to be acceptable for non-invasive imaging.
Aims: We aimed to elucidate whether serum caffeine is independently associated with adenosine-induced fractional flow reserve (FFR) overestimation and their concentration-response relationship.
Methods: FFR was measured using adenosine (FFRADN) and papaverine (FFRPAP) in 209 patients. FFRADN overestimation was defined as FFRADN − FFRPAP. The locally weighted scatterplot smoothing (LOWESS) approach was applied to evaluate the relationship between serum caffeine level and FFRADN overestimation. Multiple regression analysis was used to determine independent factors associated with FFRADN overestimation.
Results: Caffeine was ingested at <12 hours in 85 patients, at 12-24 hours in 35 patients, and at >24 hours in 89 patients. Multiple regression analysis identified serum caffeine level as the strongest factor associated with FFRADN overestimation (p<0.001). The LOWESS curve demonstrated that FFRADN overestimation started from just above the lower detection limit of serum caffeine and increased approximately 0.01 FFR unit per 1 mg/L increase in serum caffeine level with a linear relationship. The 90th percentile of serum caffeine levels for the ≤12-hour, the 12-24-hour, and the >24-hour groups corresponded to FFRADN overestimations by 0.06, 0.03, and 0.02, respectively.
Conclusions: Serum caffeine overestimates FFRADN values in a linear concentration-response manner. FFRADN overestimation occurs at much lower serum caffeine levels than those that were previously believed. Our results highlight that standardised caffeine control is required for reliable adenosine-induced FFR measurements.
Introduction
Fractional flow reserve (FFR) is widely recommended to guide clinical decision making for patients with coronary artery disease1,2. FFR is calculated using the ratio of the mean distal coronary artery pressure (Pd) to the mean aortic pressure (Pa) during pharmacologically induced hyperaemia, based on the premise that coronary pressure is linearly related to myocardial blood flow under maximal hyperaemia3. Intravenous adenosine is the standard method for hyperaemia induction both in FFR measurement and in non-invasive imaging4,5. However, several reports have indicated that the hyperaemic efficacy of adenosine is attenuated in the presence of serum caffeine6,7,8.
Caffeine antagonises the pharmacologic actions of adenosine by competitively blocking adenosine receptor activity9. Because a large majority of adults consume caffeine daily, the impact of caffeine on the accuracy of adenosine stress tests is clinically relevant. Underestimation of myocardial ischaemia severity on adenosine stress tests due to caffeine antagonism may be associated with adverse cardiac events, as suggested in non-invasive imaging studies10,11. There have been inconsistent opinions regarding the impact of caffeine on adenosine stress tests. Non-invasive imaging guidelines recommend the avoidance of caffeine for >12 or >24 hours before pharmacological stress tests12,13. In contrast, based on the results from small single photon emission computed tomography (SPECT) studies14,15, review articles concluded that caffeine intake from one cup of coffee one hour before adenosine stress tests, corresponding to serum caffeine levels of 3-4 mg/L, is acceptable16,17. The interaction between caffeine and adenosine-induced FFR measurements remains unclear. Although adenosine overestimated the FFR values compared with other stress agents in the presence of serum caffeine at lower levels than 3-4 mg/L7,18, there are several potential factors other than caffeine that are associated with adenosine-induced FFR overestimations. There is currently a lack of a widely accepted consensus concerning caffeine abstinence for FFR measurements.
We aimed to elucidate whether serum caffeine is independently associated with adenosine-induced fractional flow reserve (FFR) overestimation and their concentration-response relationship. Intracoronary papaverine induces maximum hyperaemia by directly relaxing the vascular smooth muscle, independently from caffeine18,19,20. This study compared FFR measured using adenosine (FFRADN) with FFR measured using papaverine (FFRPAP), as a reference standard, in a real-world patient population.
Methods
The study protocol was approved by the institutional ethics committee. Informed consent was obtained from all patients before the examination.
STUDY PATIENTS
This study enrolled 235 consecutive patients who underwent clinically indicated coronary angiography and FFR assessment for coronary stenosis, which was defined as 30-90% based on visual estimation during angiography. If multivessel disease was present, only the first vessel in which FFR was measured was included in this study. The exclusion criteria were acute myocardial infarction, severe arrhythmia (e.g., atrial fibrillation or frequent ectopic beats), lesions located on the coronary ostium, a prior coronary artery bypass graft, significant valvular disease, patients taking theophylline-containing medications, and patients with contraindications for adenosine or papaverine. To ensure the accuracy of the analysis, insufficient pressure data quality, such as insufficient waveform tracings and signal drift defined as FFR values of <0.97 or >1.03 after the pullback of the pressure wire, was also excluded from the analysis21.
Owing to the lack of standardised caffeine control guidelines in FFR measurements, instructions for abstinence from caffeine-containing products were at the discretion of the referring physicians. We acquired information on habitual caffeine consumption and caffeine intake within 24 hours of the FFR measurement.
FRACTIONAL FLOW RESERVE MEASUREMENTS
Coronary angiography was performed via the radial or femoral approach in multiple projections. Distal coronary pressure and aortic pressure were simultaneously measured at baseline and during maximal hyperaemia using a coronary pressure guidewire (Philips Volcano or Abbott Vascular) and a 5 or 6 Fr guiding catheter without side holes, as previously described4. Special care was taken to disengage the guiding catheter from the ostium during FFR measurements and to retain the pressure wire at the same position. Intracoronary isosorbide dinitrate (2 mg) was administered before FFR measurements.
Intravenous adenosine was continuously administered via the femoral vein or the large forearm vein at a dose of 140 μg/kg/min for a minimum of 150 seconds3,4,5,22. When steady-state hyperaemia was not obtained, adenosine infusion was maintained for a minimum of 180 seconds. After the termination of adenosine infusion, haemodynamic variables were monitored for a minimum of five minutes until they returned to the baseline level. Thereafter, intracoronary papaverine (8-10 mg in the right coronary artery or 12-15 mg in the left coronary artery) was administered through the coronary catheter, followed by 5 ml of saline3,4. The order of hyperaemic agents was determined because adenosine has a shorter half-life than papaverine5,20. FFRADN overestimation was defined as FFRADN−FFRPAP.
DATA ANALYSIS
Experienced observers blinded to the clinical information manually reviewed the pressure recordings on a beat-to-beat basis using the digital archives of device consoles6,7,18,23. Automated FFR calculation provided by the consoles was not used in this study. Pressure waveforms from ectopic beats and the adjacent beats were excluded from the analysis. FFRADN was measured during the steady-state hyperaemic plateau phase >60 seconds after the initiation of adenosine infusion24,25. When steady-state hyperaemia was not obtained during adenosine infusion, the lowest Pd/Pa value >15 seconds after the onset of the dip in Pd/Pa was taken as FFRADN24,25.
SERUM CAFFEINE CONCENTRATION
Blood samples were collected immediately before the FFR measurement. Serum caffeine concentrations were measured using liquid chromatography-mass spectrometry. The lower detection limit was 0.002 mg/L. Samples below the detection limit were regarded as 0 mg/L.
STATISTICAL ANALYSIS
Continuous variables are presented as median with interquartile ranges, unless otherwise stated. Categorical variables are presented as numbers and proportions. Patients were divided into three groups according to the time from the last caffeine intake before the test (≤12 hours, 12-24 hours, and >24 hours). Comparisons among the groups were made using the Kruskal-Wallis test. The locally weighted scatterplot smoothing (LOWESS) approach was used to evaluate the relationship between serum caffeine level and FFRADN overestimation. Simple and multiple regression analyses were performed to determine factors associated with FFRADN overestimation. Significant variables from patient and lesion characteristics and haemodynamic parameters in the simple regression model were included in the multiple regression model.
The statistical analyses were performed using JMP® Pro, version 15.0.0. (SAS Institute Inc., Cary, NC, USA). A p-value <0.05 was considered statistically significant.
Results
PROCEDURES
A total of 26 patients were excluded from the analysis - 15 due to sensor drift or insufficient waveform tracings, 6 due to sustained second-degree atrioventricular block, hypotension, or intolerable symptoms (e.g., chest pain, dyspnoea, or nausea) during adenosine infusion, 1 due to ventricular fibrillation requiring electrical cardioversion after the papaverine injection, and 4 due to an extremely tortuous vessel with heavy calcification, resulting in difficulty in advancing the pressure wire far distal to the index lesion. Finally, 209 patients were analysed in this study.
PATIENT AND LESION CHARACTERISTICS
Patient and lesion characteristics are summarised in Table 1. Most of the patients (n=192, 92%) consumed coffee or tea daily. The last caffeine intake before the test was at ≤12 hours in 85 patients (41%), at 12-24 hours in 35 patients (17%), and at >24 hours in 89 patients (43%). Serum caffeine levels were distributed widely from 0 to 9.025 mg/L (median 0.419 mg/L [interquartile range 0.098-1.203 mg/L]). Serum caffeine level decreased in proportion to the time from the last caffeine intake (0.911 mg/L [0.347-2.695] for the <12-hour group, 0.669 mg/L [0.307-1.741] for the 12-24-hour group, and 0.136 mg/L [0-0.386] for the >24-hour group; p<0.001) (Figure 1A). Likewise, FFRADN overestimation decreased with the time from the last caffeine intake (0.03 [0.01-0.05] for the <12-hour group, 0.03 [0-0.04] for the 12-24-hour group, and 0.01 [0-0.03] for the >24-hour group; p<0.006) (Figure 1B).
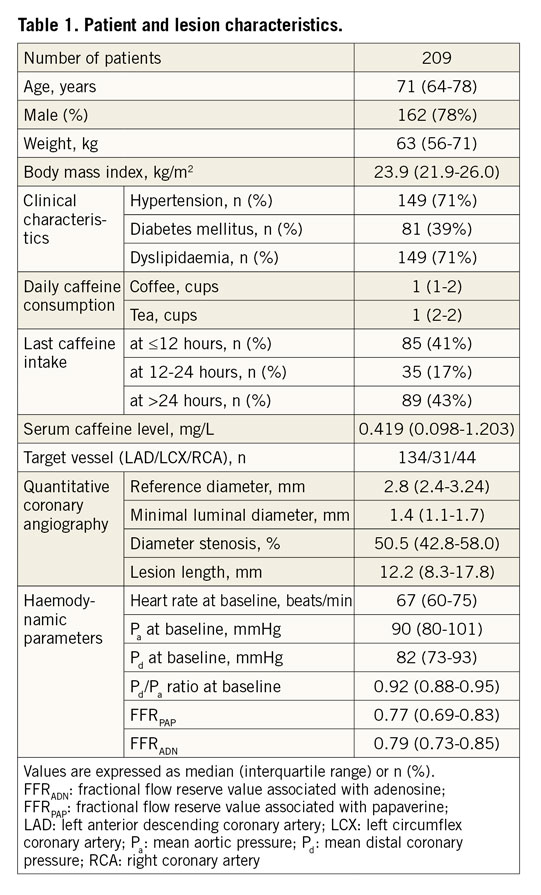
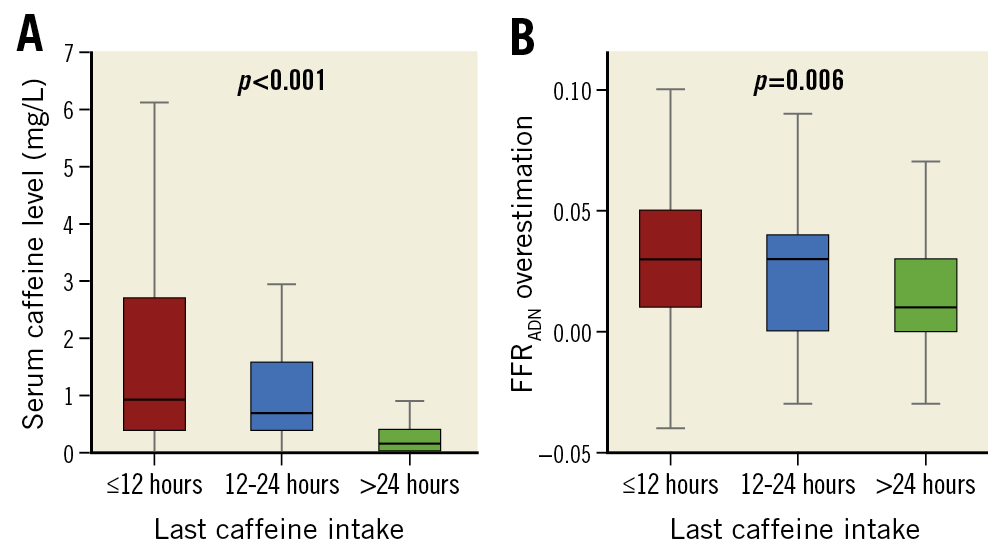
Figure 1. Comparisons among subgroups according to the time from the last caffeine intake. A) Serum caffeine level. B) FFRADN overestimation. FFRADN overestimation was defined as FFRADN−FFRPAP. FFRADN: fractional flow reserve value associated with adenosine; FFRPAP: fractional flow reserve value associated with papaverine
The distribution of FFRPAP values is shown in Figure 2. FFRPAP values were distributed within the so-called grey zone of 0.76-0-80 in 40 vessels (19%), in the adjacent strata of 0.71-0.75 in 38 vessels (18%) or 0.81-0.85 in 35 vessels (17%).
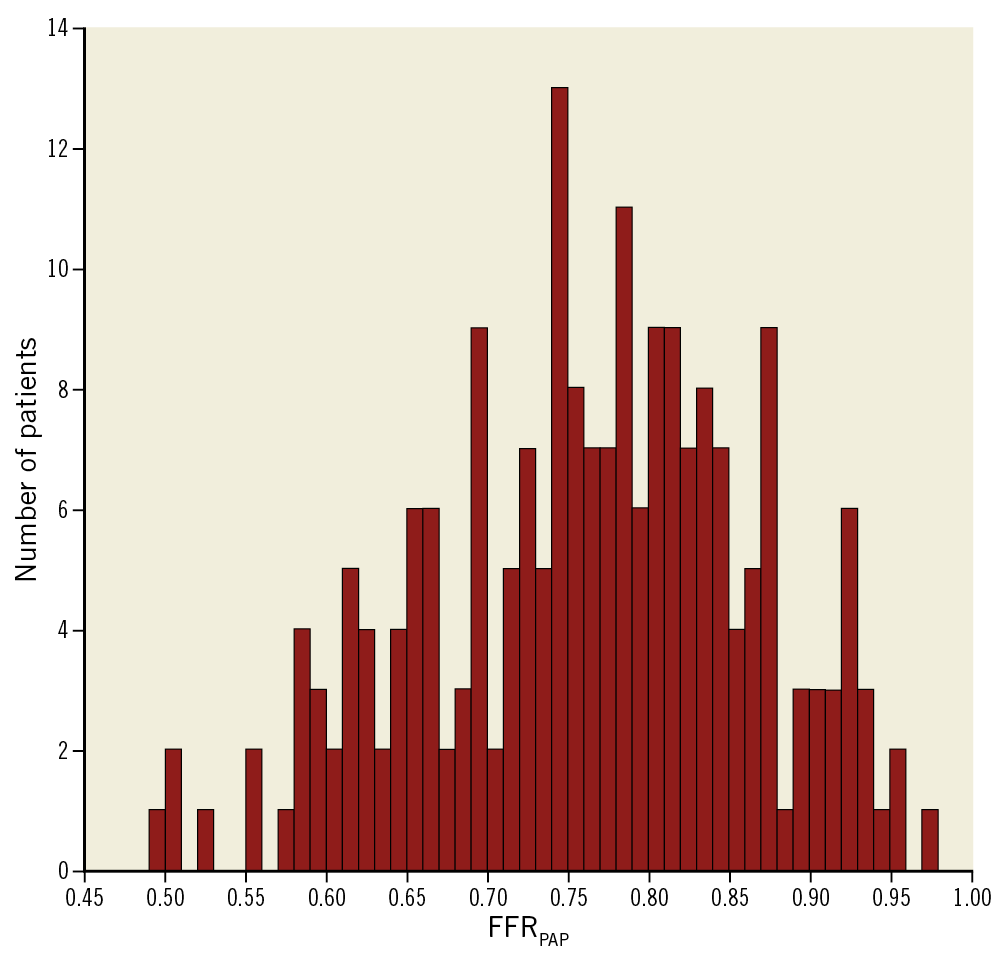
Figure 2. Distribution of FFRPAP values. FFRPAP: fractional flow reserve value associated with papaverine.
ASSOCIATION OF SERUM CAFFEINE LEVEL WITH FFRADN OVERESTIMATION
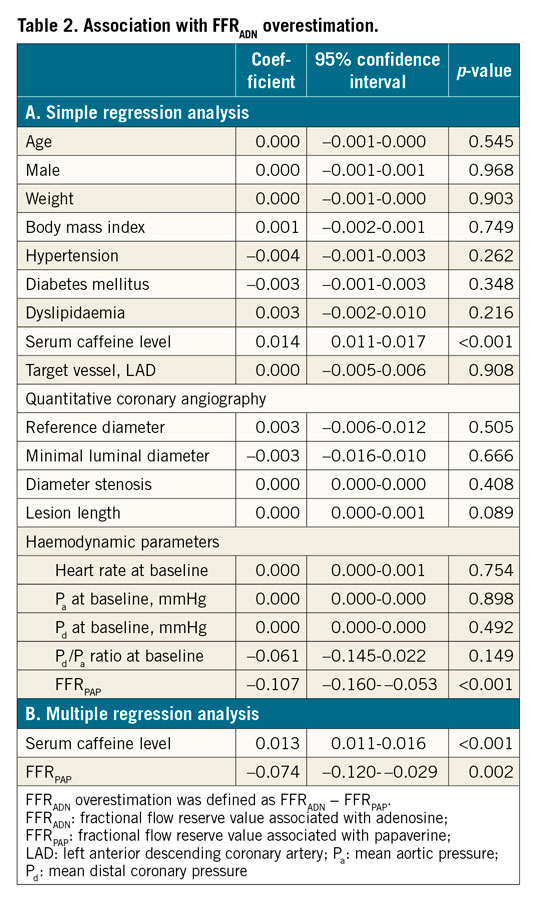
The Central illustration demonstrates the relationship between serum caffeine level and FFRADN overestimation. Simple and multiple regression analyses were applied to determine factors associated with FFRADN overestimation. The simple regression model identified serum caffeine level (p<0.001) and FFRPAP (p<0.001) as significant factors (Table 2A). Based on this result, serum caffeine level and FFRPAP were entered into the multiple model. The multiple regression analysis identified serum caffeine level to be the strongest factor associated with FFRADN overestimation (regression coefficient=0.013 [95% confidence interval: 0.011-0.016], p<0.001) (Table 2B).
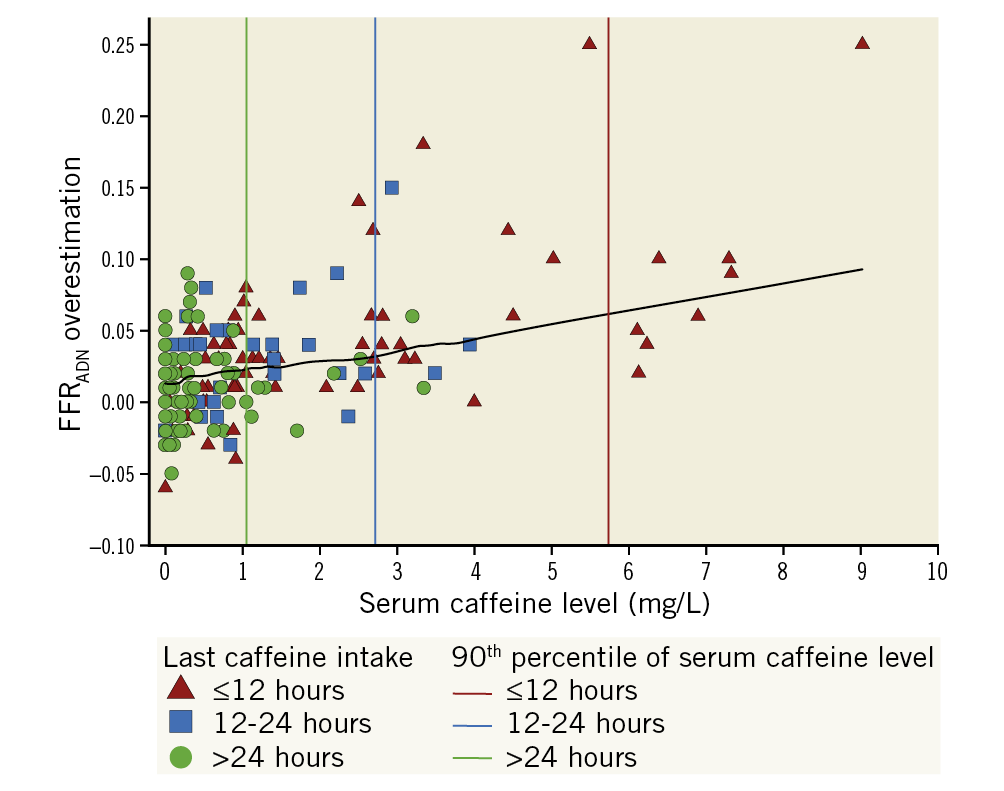
Central illustration. Relationship between serum caffeine level and FFRADN overestimation. FFRADN overestimation was defined as FFRADN−FFRPAP. The black line represents a locally weighted scatterplot smoothing curve. The red line corresponds to the 90th percentile of serum caffeine level for the ≤12-hour caffeine intake group (5.741 mg/L), the blue to the 12-24-hour group (2.722 mg/L), and the green to the >24-hour group (1.050 mg/L). FFRADN: fractional flow reserve value associated with adenosine; FFRPAP: fractional flow reserve value associated with papaverine
The LOWESS curve indicated an approximately linear concentration-response relationship of serum caffeine level with FFRADN overestimation. FFRADN overestimation started from just above the lower detection limit of serum caffeine and increased approximately 0.01 FFR unit per 1 mg/L increase in serum caffeine level. Serum caffeine levels of 3-4 mg/L that are considered acceptable for SPECT resulted in an FFRADN overestimation of approximately 0.04. The 90th percentile of serum caffeine levels for the ≤12-hour group (5.741 mg/L), for the 12-24-hour group (2.722 mg/L), and for the >24-hour group (1.050 mg/L) corresponded to FFRADN overestimations by 0.06, 0.03, and 0.02, respectively.
REPRODUCIBILITY OF SERUM CAFFEINE LEVEL
Serum caffeine level was measured twice in 20 randomly selected blood samples in the study population to assess the reproducibility of measurements. The reproducibility of measuring the serum caffeine level was excellent, with a correlation coefficient of 0.999 (p<0.001).
Discussion
Evaluating the relationship between serum caffeine levels and FFRADN overestimation, we demonstrated the following findings: 1) FFRADN overestimation increased linearly with increasing serum caffeine level (approximately 0.01 FFR unit per 1 mg/L increase in serum caffeine level), starting from much lower levels than those that were previously considered acceptable for SPECT; 2) serum caffeine levels of 3-4 mg/L considered acceptable for SPECT caused FFRADN overestimation of approximately 0.04; and 3) serum caffeine level was the strongest factor associated with FFRADN overestimation.
ASSOCIATION BETWEEN SERUM CAFFEINE LEVEL AND FFRADN OVERESTIMATION
This study, conducted on the largest number of patients to date, is the first to demonstrate a linear concentration-response relationship between serum caffeine and FFRADN overestimation. Given caffeine’s role as a competitive adenosine receptor antagonist, the concentration-response relationship stands to reason. It should be noted that FFRADN overestimation started at just above the detection limit of serum caffeine, which was much lower than that which was previously believed acceptable for SPECT16. Our results underscore the need for strict caffeine control to avoid FFRADN overestimation (as discussed in the “Importance of caffeine abstinence before FFR measurements” section).
The present study identified serum caffeine level and FFRPAP to be significant factors associated with FFRADN overestimation. The result is reasonable from a physiological point of view. A lesion with a low FFR value has a large discrepancy between FFRADN and FFRPAP when adenosine fails to induce maximal hyperaemia due to caffeine antagonism. In a SPECT study using regadenoson, a selective A2A receptor agonist, the effect of caffeine on reversible perfusion defects was more evident in patients with extensive abnormalities26. The strongest association of serum caffeine with FFRADN overestimation in the multiple model consolidates our conclusion.
COMPARISON WITH NON-INVASIVE IMAGING
Reyes et al showed that two cups of coffee consumed one hour before testing reduced the magnitude of adenosine-induced perfusion abnormalities on SPECT8. Research by Zoghbi et al and Lee et al revealed that one cup of coffee did not have this effect14,15. The mean serum caffeine level in the study by Reyes et al was higher (6.2 mg/L) than that in the studies by Zoghbi et al and Lee et al (3.1 mg/L and 3.4 mg/L). Based on these results, serum caffeine levels of 3-4 mg/L have been considered acceptable for adenosine SPECT16. In contrast, the present study revealed that FFRADN overestimation was observed at much lower levels than 3-4 mg/L, which was in line with the finding of a prior FFR study7.
The inconsistent results between FFR and SPECT studies are presumably due to differences in methodology. Unlike relative SPECT perfusion imaging, FFR expresses the maximum achievable blood flow in a stenotic artery as a fraction of the theoretical normal maximum blood flow in the same vessel3. We used FFRPAP as the reference18,19,20, which is not affected by caffeine. SPECT studies compared two separate adenosine tests (with 24-hour caffeine abstinence versus one hour after caffeine ingestion)14,15. Non-negligible serum caffeine levels (0.03-1.79 mg/L) in the scans with caffeine abstinence might obscure the effect of the caffeine intervention15. Additionally, these negative results could be attributed to a small sample size (n=30). Another explanation would be the well-known roll-off phenomenon observed in non-invasive perfusion imaging27. Myocardial blood flow supplied by a normal coronary artery increases threefold to fivefold during adenosine stress, compared with that at baseline. The uptake of tracers increases in proportion to myocardial blood flow at lower levels and reaches a maximum of approximately 2.5 times28. The results on adenosine stress SPECT cannot, therefore, be altered unless caffeine decreases the adenosine-induced augmentation of uptake to below the maximum. Higher caffeine levels would be required to exert a significant effect on adenosine-induced perfusion defect on SPECT. These could explain, in part, the discrepancies between FFR and SPECT studies.
IMPORTANCE OF CAFFEINE ABSTINENCE BEFORE FFR MEASUREMENTS
In addition to time from caffeine intake, there are several factors that affect serum caffeine level, including habitual caffeine consumption, caffeine concentration or dose in food or beverage recently ingested, and inter-individual variation in half-life (ranging from 2 to 12 hours). Nevertheless, decreases in FFRADN overestimation, as well as serum caffeine level, with the time from caffeine intake suggest the significance of adequate time for caffeine control. Because FFR is the gold standard for functional significance assessment, no “acceptable” FFRADN overestimation exists. Considering that a standard deviation for repeated FFRADN measurements is 0.0225 and that the 90th percentile of serum caffeine levels for ≤12-hour, 12-24-hour, and >24-hour caffeine intake causes FFRADN overestimation by 0.06, 0.03, and 0.02, respectively, at least 24-hour caffeine avoidance is recommended. More prolonged caffeine avoidance for >48 hours could achieve zero serum caffeine levels in most cases7. However, such strict caffeine control for all patients who are scheduled to undergo invasive angiography is impractical in routine care, and should be considered for certain subgroups of individuals who habitually consume large amounts of caffeine or who have a prolonged caffeine half-life, such as individuals with liver disease.
CLINICAL IMPLICATIONS
Pharmacologic, non-invasive myocardial perfusion imaging studies have suggested that serum caffeine might influence patient management, leading to adverse cardiovascular events10,11. The same may be true for FFR measurements. Caffeine’s antagonism to adenosine underestimates patients’ risk as FFR is linearly associated with subsequent adverse cardiac events29. FFR overestimation may result in missing a chance to receive benefits from revascularisation. Furthermore, FFRADN overestimations due to divergent caffeine control practices hamper comparisons within and across FFR studies.
Currently, no standardised guideline exists concerning caffeine abstinence for FFR measurements. As such, in daily clinical practice, not all referring physicians instruct patients scheduled for invasive coronary angiography to abstain from caffeine intake. Thus, clinicians must be aware of the need for caffeine abstinence, and patients should be fully informed of the wide range of dietary caffeine sources. Caffeine abstinence, however, is not possible in the acute setting, and inadvertent caffeine intake is not uncommon in daily clinical practice. In such cases, hyperaemic stimuli unaffected by caffeine (e.g., papaverine and nicorandil) or recently well-validated non-hyperaemic coronary pressure indices should be considered as alternatives4,18,19,30. A rapid test kit to detect serum caffeine, if available, would be useful to determine if adenosine should be used.
Study limitations
We acknowledge some limitations in our study. First, the study was conducted only on a Japanese population; therefore, potential ethnic biases cannot be excluded. Second, this study did not assess coronary flow as clinical guidelines have provided the highest recommendation for coronary pressure assessments for the evaluation of physiological significance1,2. Coronary flow and microcirculatory resistance measurements would provide more insights into this subject. Finally, the order of hyperaemic agents was not randomised (adenosine first). Despite adenosine’s short half-life5, its carry-over effect cannot be excluded.
Conclusions
Serum caffeine causes adenosine-induced FFR overestimation in a linear concentration-response manner. Adenosine-induced FFR overestimation occurs even at much lower serum caffeine levels than those that were previously believed acceptable for non-invasive imaging. Our results highlight the need to standardise adequate caffeine control for reliable adenosine-induced FFR measurements.
|
Impact on daily practice Adenosine-induced fractional flow reserve (FFR) is the gold standard for assessing the physiological significance of coronary artery stenosis. Insufficient hyperaemia, however, causes FFR overestimation, leading to inappropriate patient management. Because caffeine is a competitive antagonist of adenosine, it is important to determine its impact on the accuracy of adenosine-induced FFR measurements. Thus far, there is no consensus regarding caffeine abstinence for FFR measurements. This study demonstrated an approximately linear relationship between serum caffeine level and adenosine-induced FFR overestimation, starting from much lower levels than those that were previously believed acceptable. Multiple regression analysis confirmed serum caffeine level as the strongest factor associated with adenosine-induced FFR overestimation. Our results highlight that the importance of standardised caffeine control for reliable adenosine-induced FFR measurements. |
Acknowledgments
The authors are grateful to Professor Eisuke Inoue, PhD, at the Research Administration Center, Showa University, for his statistical advice with this paper.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.