Article Text

Abstract
Objective The Familial Hypercholesterolaemia Case Ascertainment Tool (FAMCAT) has been proposed to enhance case finding in primary care. In this study, we test application of the FAMCAT algorithm to describe risks of familial hypercholesterolaemia (FH) in a large unselected and ethnically diverse primary care cohort.
Method We studied patients aged 18–65 years from three contiguous areas in inner London. We retrospectively applied the FAMCAT algorithm to routine primary care data and estimated the numbers of possible cases of FH and the potential service implications of subsequent investigation and management.
Results Of the 777 128 patients studied, the FAMCAT score estimated between 11 736 and 23 798 (1.5%–3.1%) individuals were likely to have FH, depending on an assumed FH prevalence of 1 in 250 or 1 in 500, respectively. There was over-representation of individuals of South Asian ethnicity among those likely to have FH, with this cohort making up 41.9%–45.1% of the total estimated cases, a proportion which significantly exceeded their 26% representation in the study population.
Conclusions We have demonstrated feasibility of application of the FAMCAT as an aid to case finding for FH using routinely recorded primary care data. Further research is needed on validity of the tool in different ethnic groups and more refined consideration of family history should be explored. While FAMCAT may aid case finding, implementation requires information on the cost-effectiveness of additional health services to investigate, diagnose and manage case ascertainment in those identified as likely to have FH.
- hyperlipidaemias
- coronary artery disease
- delivery of healthcare
- electronic health records
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplemental information. Data are extracted from patient record systems held by GP practices. Outputs of the data extracted are collated and in the format of tables within the paper or in supplemental information.
Statistics from Altmetric.com
Introduction
The National Health Service (NHS) Long Term Plan is committed to reducing cardiovascular disease with an ambition to prevent 150 000 strokes, heart attacks and dementia cases over 10 years by detecting and treating risk factors including hypercholesterolaemia.1 Ischaemic heart disease (IHD) and strokes are among the most common causes of death in the UK2 with particularly high risks where the median age-standardised prevalence of hypercholesterolaemia (>6.2 mmol/L) exceeds 20%.3 The Global Burden of Disease Study and the WHO Global Action Plan highlight that reduction of premature cardiovascular mortality is an international priority.4 5
Familial hypercholesterolaemia (FH) is a genetic disorder characterised by elevated serum low-density lipoprotein cholesterol (LDL-C).6 7 In individuals of European descent, FH is associated with a 10-fold greater lifetime risk of IHD and early death.8 Diagnosis is through clinical evaluation with validated diagnostic criteria (Simon Broome (SB) or Dutch Lipid Clinic Network (DLCN)) and consideration of genetic testing.9 Global cardiovascular risk scores are not applicable to patients with FH as they are already at high risk of IHD.8 10 Evidence supports early treatment in substantially reducing the risk of FH-related IHD and mortality. For patients with an inadequate response to standard therapies, there are expanded options from secondary care including PCSK9 inhibitors and new-in-class drugs.11–14 However, over 75% of estimated FH cases are undiagnosed15 16 representing a missed opportunity to reduce the burden of cardiovascular disease.
Existing approaches to case finding of FH in primary care are suboptimal. The National Institute of Clinical Excellence advises assessment of people considered at high risk of FH based on total cholesterol levels or reported family history.10 Time and resource constraints in primary care precludes application of the SB and DLCN assessment consistently and completely in large numbers of patients. Therefore, current approaches to case finding are associated with significant inaccuracies and have the potential for underdiagnosis of FH and referral of high numbers of false positives.
The FH Case Ascertainment Tool (FAMCAT) is an externally validated case finding tool to identify individuals likely to have FH through systematic searching of routine primary care records for lipid profiles and other contributory variables.17 18 Subsequent targeting of detailed clinical assessments to those at highest risk could enable more appropriate use of limited clinical resources, greater accuracy in identification of cases and improvement in case finding coverage.19 20 Estimates of the cohort size allow for service planning and commissioning intentions, including primary care workload, demand for genetic testing and development of specialist clinics.
Objective
In this study, we retrospectively applied the FAMCAT to an unselected population of over 770 000 primary care patients aged 18–65 years in East London, UK, using routinely collected primary care data. We report on the risk stratification of the population by FAMCAT and the number of cases identified as likely to have FH, requiring further clinical assessment.
Methods
Study setting
The analysis dataset included all primary care patients aged 18–65 years registered with general practitioners within three Clinical Commissioning Groups (CCGs) in East London. This comprised 127 practices (City and Hackney, n=42; Newham, n=50; Tower Hamlets, n=35), which use the Egton Medical Information Systems (EMIS) electronic health record. Compared with UK averages, this inner urban population has a greater proportion of individuals from black, South Asian and minority ethnic groups, younger average age, and higher levels of socioeconomic deprivation. In these CCGs, implementation of primary and secondary cardiovascular disease prevention strategies is higher than the national average. However, local levels of cardiovascular morbidities, in particular, premature cardiovascular disease, are ranked in the top 10% in the UK.21
Defining the study population
We included men and women aged 18–65 years old registered with a participating practice at the time of data extraction (01 July 2019). As FH is associated with premature IHD, we set the upper age limit as 65 years old. De-identified data based on Read codes in EMIS records were extracted centrally by the Clinical Effectiveness Group, Queen Mary University of London, including age, sex, ethnicity, clinical conditions (online supplemental table 1) and social deprivation. Deprivation was defined by national 2015 Index of Multiple Deprivation (IMD) quintiles derived from a geographical area comprising approximately 150 households. Blood pressure (BP) and smoking status were defined based on their most recent records. Ethnic group is self-reported and recorded in the health records and then categorised as black ethnicity including black African, Caribbean and black British; South Asian including Bangladeshi, Pakistani, Indian and other Indian subcontinent; white including white British and European; and other ethnic group including missing or not stated.
Supplemental material
Definition of the FAMCAT variables
The FAMCAT score was devised and externally validated by Weng et al.17 In this study, we matched our definitions of the FAMCAT variables as closely as possible with that of the original (online supplemental table 2). For cholesterol, we considered the highest ever recorded value and if both total cholesterol and LDL-C were available, we gave preference to LDL-C. The highest triglyceride measured within 5 years of the highest cholesterol was used. In cases of missing triglyceride and/or cholesterol data, we used the mean value of the analysis sample based on patient’s sex, age group of either <40 years or ≥40 years and the IHD status. In alignment with Weng et al,17 outlying observations of cholesterol and triglyceride levels and data entry errors were excluded. We classed levels as ‘untreated’ if there was no record of prescription for lipid-lowering drugs (statin, fibrate, bile acid sequestrant, nicotinic acid) in the 90 days prior to cholesterol measurement. We categorised potency of lipid-lowering therapy into low (fluvastatin or pravastatin ≤ 40 mg/day; simvastatin ≤ 10 mg/day), medium (fluvastatin or pravastatin 80 mg/day; simvastatin 20 mg/day or 40 mg/day; atorvastatin ≤ 10 mg/day; rosuvastatin 5 mg), or high (simvastatin 80 mg; atorvastatin ≥ 20 mg/day; rosuvastatin ≥ 10 mg/day) intensity.
Supplemental material
Calculation of FAMCAT risk
FH risk was calculated through application of the FAMCAT regression equations to our study population with variables defined as outlined. Estimates were based on probability thresholds of both 1 in 250 and 1 in 500 population prevalence of FH.16 22 We categorised risk stratification resulting from this analysis as unlikely, may or likely to have FH. A relative population risk of <1 indicated the individual was unlikely to have FH, a relative population risk from 1 to 5 indicated the individual may have FH, and a relative population risk of >5 indicated the individual is likely to have FH. We present these results for the whole cohort and separately for individuals with premature IHD (onset before age 65 years).
We performed a sensitivity analysis without imputations using the other variables to estimate the risk of FH where cholesterol and triglyceride were missing (see online supplemental table 3).
Patient and public involvement
Patients and the public were not involved in the design, conduct or outcome of this work.
Results
Baseline population characteristics
The analysis sample comprised 404 657 women and 372 471 men with mean age (SD) of 37.2 (11.6) years (range 18–65 years). The population was ethnically diverse including white (308 694, 39.7%), South Asian (201 957, 26.0%), and black Caribbean and African (104 138, 13.4%) ethnic groups (table 1). Levels of deprivation were high relative to UK national averages with >90% of patients in the two most deprived IMD quintiles. The prevalence of smoking, diabetes, hypertension, chronic kidney disease (CKD) and stroke were 157 549 (20.3%), 42 844 (5.5%), 59 215 (7.6%), 11 629 (1.0%) and 3500 (0.5%), respectively. Prevalence of pre-existing IHD was 7950 (1.0%), with IHD recorded prior to the age 60 years in 6444 (81%) of these patients.
Characteristics of the study population aged 18–65 years and the characteristics of the FAMCAT derivation cohort aged 16 years or above
Level of recording of required data
Table 2 shows the level of data recording. Cholesterol was recorded for 82.5% (6558) of patients with IHD and 39.5% (303 921) of patients without IHD. Of the 16 573 with coded FH, 14.5% (2,397) did not have cholesterol recorded. Recording of cholesterol was more frequent for individuals aged 40 years and older.
Completeness of data recording
FAMCAT risk applied to the whole cohort
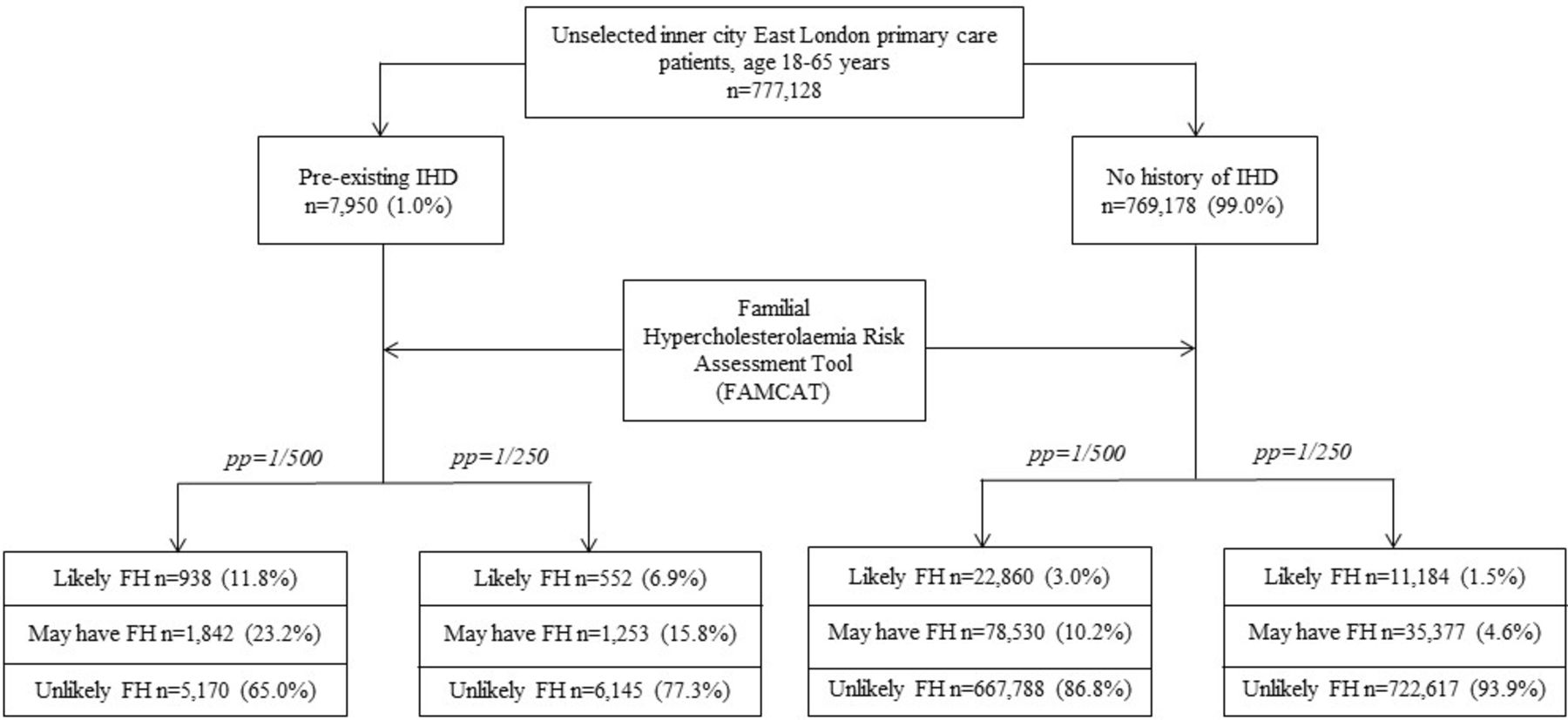
Within the study population (777 128), 11 736–23 798 (1.5%–3.1%) patients were estimated to be likely to have FH, depending on the prevalence assumed (figure 1). A total of 36 630–80 372 (4.7%–10.3%) patients were estimated they may have FH (table 3). For individuals with IHD (7950), 552–938 (6.9%–11.8%) were likely to have FH and 1253–1842 (15.8%–23.2%) may have FH. For those without IHD (769 178), 11 184–22 860 (1.5%–3.0%) were likely to have FH. In total, between 48 366 and 104 170 people were estimated that they may or were likely to have FH who may need further investigation (between 6.2% and 13.4% of our total cohort). The computation of FAMCAT risk with and without missing data for both IHD and non-IHD resulted in changes of less than 1% in all categories of risk (online supplemental table 3).

{kind=link}
Risk of familial hypercholesterolaemia (FH) in inner East London calculated using FAMCAT algorithm, assuming population prevalence of 1 in 500 and 1 in 250. IHD, ischaemic heart disease; PP, population prevalence.
Predicted number of cases of familial hypercholesterolaemia assuming population prevalence of 1 in 500 and 1 in 250
FAMCAT risk in ethnic groups
Table 4 describes risk of FH by ethnic group. A total of 39.7% of the study population were in white ethnic groups. Among individuals of white ethnicity who had IHD, 7.8%–13.2% were estimated they were likely to have FH, compared with 6.8%–11.6% of South Asians and 5.2%–9.9% of black African/Caribbean individuals. In white ethnic groups without IHD, 1.2%–2.5% were likely to have FH compared with 2.5%–4.8% in South Asian and 1.1%–2.8% in black African/Caribbean groups.
Comparison of risk of FH estimated by FAMCAT by ethnicity
Discussion
In this large study of 777 128 primary care patients, we demonstrated the feasibility of application of the FAMCAT algorithm to aid case finding of FH using routinely recorded primary care data. Our analysis identified between 48 366 and 104 170 (6.2%–13.4%) people who may or were likely to have FH who would therefore warrant further assessment and potentially genetic testing and specialist services. These findings have important implications for care and service planning in primary and secondary care.
In our population, 1 in 30 to 1 in 100 were likely to have FH according to FAMCAT risk stratification, compared with estimates of disease prevalence from 1 in 250 to 1 in 500.16 22 Among individuals with pre-existing IHD, this increased to 6.9%–11.8%, suggesting that targeting testing and treatment for FH in this latter group would have a higher positive case yield.19 20
A total of 2.1% of this population were found to have a code for FH, which is higher than previously reported estimates of FH prevalence. The prevalence in our study may be inflated due to coding errors where patients with high cholesterol and/or family history of high cholesterol were incorrectly coded as ‘FH’ without further scrutiny to determine a correct diagnosis. Of those coded as having FH, 47.5% were identified by FAMCAT as unlikely to have FH (online supplemental table 4). Further clarification on the accuracy of these diagnoses is needed. This would require a case note review, which was not available in this study.
FAMCAT in ethnic groups
The risk of FH varied by ethnicity. In those with IHD, FH likelihood was highest in white and lowest in black ethnic groups. In people without IHD, the FH likelihood was highest in South Asian and lowest in black groups. This may suggest that FH is a more important factor in development of IHD for white ethnicities. Alternatively, our observations may indicate lower sensitivity of FAMCAT in detecting FH in black and South Asian ethnic groups. Indeed, lower predictive accuracy of the FAMCAT in these groups has been previously highlighted.18 Further research is needed on potential ethnicity differential disease patterns of FH and the performance of risk prediction tools including the FAMCAT for informed clinical application in ethnically diverse populations.
Comparison with FAMCAT validation population
The FAMCAT validation population17 ran from 1999 to 2013, while our population was more contemporaneous comprising those currently registered in 2019. Our population was, on average, younger than that studied by Weng et al, with a mean age of 37.2 vs 49.5 years.17 The average age at first cholesterol measurement was higher in the Weng et al cohort (57 vs 35.7 years) as was the prevalence of diabetes and CKD (12.8% vs 5.5%, 11.7% vs 1.5%), which is likely to be due to older age of participants in their cohort. There is a difference in the mean total cholesterol, while the mean LDL is similar between our study populations. However, the standard deviations of the means overlap, indicating that this difference is not statistically significant. Our population had a higher proportion of people with a recorded family history of myocardial infarction: 19.6% vs 3.2% in the Weng et al cohort. Recording of family history is integral to the national NHS Health Check programme in East London which may be the main reason for high levels of documentation, though the accuracy of these recordings is unknown.23 FAMCAT only considers family history of IHD as a binary score and does not consider kinship or prematurity of onset. The relevance of accurate family history of premature IHD is an outstanding issue for further research as it is an essential element of further case identification. A comparison cannot be made between ethnicity and deprivation as they were not reported in the Weng et al paper. In keeping with Weng et al, patients on ezetimibe alone had their levels classed as ‘untreated’. We also observed less missingness in all variables of interest for individuals aged over 40 years, corresponding to the 40–74 years of eligibility threshold for the NHS Health Check since 2009 and the inclusion of BP in the national Quality and Outcomes Framework for people over 40 years since 2013.
Implications for clinical practice
The 23 798 patients who were likely to have FH represent a large group of patients within which FH cases may exist, and these have been relatively easily identified through a data-driven approach. Use of the FAMCAT algorithm could allow primary care practices to generate a list of patients who may have FH, where the diagnosis has not yet been considered or excluded, using routinely recorded data. These at-risk individuals could be reviewed in more detail to determine an up-to-date FAMCAT risk and, if appropriate, clinical evaluation using the DLCN or SB criteria and genetic testing to confirm their disease status.
FAMCAT has showed a high degree of discrimination (area under the receiver operating curve 0.832, 95% CI 0.820 to 0.845). Assuming a population frequency of 1 in 500, FAMCAT had a sensitivity of 84% (1028 predicted vs 1219 observed cases) and specificity of 60% (443 949 predicted vs 745 781 observed non-cases), with a positive predictive value of 0.84% and a negative predictive value of 99.2%.18 In other words, for every 119 people likely to have FH, after further investigation, 1 person would be identified with FH and 118 would not have genetically confirmed FH but would nevertheless require clinical advice on whether further treatment was required based on the family history and clinical findings.
This study demonstrates that other localities could potentially use FAMCAT to aid FH case finding, though not all areas have the digital maturity to run algorithms across the entire local population. The application of FAMCAT is likely to generate substantial additional workload for primary and secondary care services. Therefore, it is imperative to consider infrastructure requirements to accommodate the expected increase in demand in both community and secondary care settings. For instance, development of dedicated community FH facilities may be of value to reduce the burden on existing hospital lipid clinics. Such large-scale changes to specialist investigations would require evidence of cost-effectiveness and substantial changes to current care pathways.
Those who have not had an ischaemic cardiac event but are deemed likely to have FH by FAMCAT represent a group who may not otherwise have been identified before an index myocardial infarction or stroke, and for whom testing and treatment would play an important part in positively altering their disease trajectory. An FH diagnosis will help ensure they have appropriate treatment, and is also important for their families and cascade testing. In those who have had a cardiac event, confirmation of FH would have similar implications including for first-degree relatives.
Limitations
FAMCAT is not diagnostic, it merely applies a risk estimate. As seen in this paper, this approach generates a large cohort who need further scrutiny, first in primary care with a detailed family history and examination, then in secondary care for genetic testing and clinical advice. The FAMCAT algorithm generates substantial numbers at high FH risk for further investigation and management, and this process has yet to be assessed for cost-effectiveness.
Calculating individual FH risks without cholesterol and triglyceride measurements assumes values that fall into the ideal category in the FAMCAT algorithm. This could lead to incorrect estimates. Hence, we imputed missing values using population means for IHD and non-IHD groups. This approach artificially reduces the overall variability of missing variables. In studies where the primary purpose is hypothesis testing, this approach to imputation may lower the threshold for achieving statistical significance. However, this limitation is less important for this study, as the purpose of our work is demonstration of feasibility and description of the FAMCAT.
Use of the FAMCAT relies on recording of coded data including BP, cholesterol and family history. There was less missingness of these variables for individuals aged over 40 years old, notably of cholesterol. This is likely due to the NHS Health Check and suggests this could also be an opportunity to estimate the FAMCAT risk. A total of 60.5% of patients without IHD and 14.5% with IHD did not have a record of cholesterol measurement. A complete lipid profile is advisable for optimal accuracy of FAMCAT.
Conclusion
We were able to implement the FAMCAT algorithm across entire localities to estimate likely numbers of patients requiring investigation for FH and assist commissioners and health service providers to determine these approaches. However, further research on the external validity in different settings and populations is warranted for the tool to be applied more widely. The recording of key variables including first-degree family history of premature IHD and the missing data requires improvement for use in service settings. Such data-driven approaches have the potential to improve detection of FH in the general population and reduce cardiovascular morbidity and mortality, but evidence of cost-effectiveness for full implementation of such a pathway is currently lacking.
Key messages
What is already known on this subject?
Underdiagnosis of familial hypercholesterolaemia (FH) represents a significant missed opportunity for prevention of coronary artery disease and premature death. The FH Risk Ascertainment Tool (FAMCAT) is designed to improve case finding in primary care but has not been studied in unselected primary care settings.
What might this study add?
The original FAMCAT Study used a national dataset of selected volunteer practices to estimate likelihood of FH from routine data in primary care electronic health records. Our study applies FAMCAT to a large, unselected and ethnically diverse urban population. We estimate the number of people with possible FH and their demographic and clinical characteristics.
How might this impact on clinical practice?
We demonstrated that FAMCAT could be feasibly applied to routine primary care data to enhance identification of individuals with FH. This information informs planning of health service provision and highlights recording of family history and ethnicity as topics for further research and improvement.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplemental information. Data are extracted from patient record systems held by GP practices. Outputs of the data extracted are collated and in the format of tables within the paper or in supplemental information.
Ethics statements
Ethics approval
This study is based on de-identified information obtained from routinely compiled general practitioner electronic health records and did not require ethics committee approval.
Acknowledgments
We are grateful to the general practitioners and their practice teams for allowing the use of their patient records, to the Clinical Effectiveness Group for providing access to their curated high-quality dataset and to the population in East London from whom the data are derived. This work was supported by Barts Charity and Health Data Research UK, an initiative funded by UK Research and Innovation, Department of Health and Social Care (England) and the devolved administrations, and leading medical research charities.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JR and CC conceived the study. CW conducted the data extraction and the analysis. All authors contributed to the planning of the study and the manuscript.
Funding This study received no specific funding. JR, SR, CW and CC are employed by Queen Mary University of London. AT was and RSP is employed by Barts Health Trust. SR was supported by Barts Charity, JR and CW were supported by Health Data Research UK. ZR-E is supported by a British Heart Foundation Clinical Research Training Fellowship (FS/17/81/33318).
Competing interests RSP reports personal fees from SANOFI, grants from AMGEN, and personal fees from NOVARTIS, outside the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- Cardiac risk factors and prevention