Article Text

Abstract
Objective Decreased kidney function increases cardiovascular risk and predicts poor survival. Estimated glomerular filtration rate (eGFR) by creatinine may theoretically be less accurate in the critically ill. This observational study compares long-term cardiovascular mortality risk by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) creatinine equation; Caucasian, Asian, paediatric and adult cohort (CAPA) cystatin C equation and the CKD-EPI combined creatinine/cystatin C equation.
Methods The nationwide study includes 22 488 intensive care patients in Uppsala, Karolinska and Lund University Hospitals, Sweden, between 2004 and 2015. Creatinine and cystatin C were analysed with accredited methods at admission. Reclassification and model discrimination with C-statistics was used to compare creatinine and cystatin C for cardiovascular mortality prediction.
Results During 5 years of follow-up, 2960 (13 %) of the patients died of cardiovascular causes. Reduced eGFR was significantly associated with cardiovascular death by all eGFR equations in Cox regression models. In each creatinine-based GFR category, 17%, 19% and 31% reclassified to a lower GFR category by cystatin C. These patients had significantly higher cardiovascular mortality risk, adjusted HR (95% CI), 1.55 (1.38 to 1.74), 1.76 (1.53 to 2.03) and 1.44 (1.11 to 1.86), respectively, compared with patients not reclassified. Harrell’s C-statistic for cardiovascular death for cystatin C, alone or combined with creatinine, was 0.73, significantly higher than for creatinine (0.71), p<0.001.
Conclusions A single cystatin C at admission to the intensive care unit added significant predictive value to creatinine for long-term cardiovascular death risk assessment. Cystatin C, alone or in combination with creatinine, should be used for estimating GFR for long-term risk prediction in critically ill.
- epidemiology
- biomarkers
- epidemiology
Data availability statement
The datasets generated during and/or analysed during the current study are not publicly available due to the reason that the datasets used contain information that potentially could identify individual patients. Authors are willing to share their data on reasonable request and after case-by-case assessment of such request by a local ethics committee.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Glomerular filtration rate (GFR) is the best available indicator for kidney function and essential for detection and management of acute kidney injury (AKI) and chronic kidney disease (CKD). CKD, defined as GFR <60 mL/min/1.73 m2, is emphasised as a serious cardiovascular risk factor with high mortality risk in clinical guidelines including patients with kidney disease,1 hypertension, diabetes and the general population.2 A large number of critically ill patients have varying underlying cardiovascular risk factors3 including CKD and are at risk of acute kidney disease. Creatinine is the major tool for estimating GFR (eGFR) in almost all patient populations, including in the intensive care unit,4 despite the well-known risk of eGFR overestimation because of loss of muscle mass, poor meat intake and altered distribution volume due to illness. Cystatin C may serve as an alternative eGFR biomarker since it does not depend on muscle mass and protein intake but may be influenced by other factors in the critically ill, such as endogenous cortisol.5 Moreover, eGFR equations that incorporate both creatinine and cystatin C may be more closely associated with directly measured GFR than equations based on each biomarker alone.6 7 The role of creatinine and cystatin C in predicting cardiovascular mortality is less studied in critically ill patients.
The aim of this study was to investigate if cystatin C improves the association between eGFR and cardiovascular mortality in critically ill patients at intensive care, compared with creatinine, using reclassification and model discrimination with C-statistics. A large number of intensive care patients from three Swedish university hospitals with creatinine and cystatin C analysed at admission were included and followed up for a median of 5 years after discharge for long-term cardiovascular mortality risk assessment.
Methods
Study population
This observational study includes patients in intensive care units at Uppsala, Karolinska and Lund University Hospitals, from 2004 to 2015, who had both plasma creatinine and cystatin C simultaneously analysed. The samples were collected in the same tube and immediately analysed at Uppsala, Karolinska and Lund University Hospital laboratories, respectively. Adult patients, 16 years of age and older, with a complete personal identity number were included. Valid results of creatinine, cystatin C, age, gender and sampling date were retrieved from the laboratory information systems and only the first measurement was included. Thus, 22 488 unique patients with simultaneous measurements of plasma creatinine and cystatin C were included in the study. All methods were carried out in accordance with relevant guidelines, and regulations and reporting followed the Strengthening the Reporting of Observational Studies in Epidemiology checklist.
Patient and public involvement
Patients and the public were not involved in this research; this study is based on registry data and data from laboratory information systems.
Measurement of creatinine, cystatin C and eGFR
Plasma creatinine in µmol/L was analysed with isotope dilution mass spectrometry (IDMS)calibrated methods: in Uppsala Hospital laboratory with a modified kinetic Jaffe method 2004–2008 and an enzymatic method 2009–2015 on Architect ci8200 (Abbott Laboratories, Abbott Park, Illinois, USA); in Karolinska laboratory with a modified kinetic Jaffe method on UniCel DXC800 (Beckman Coulter, Brea, California, USA); in Lund with an enzymatic method on Roche Cobas c501 (Roche Diagnostics, Rotkreuz, Switzerland). Plasma cystatin C in mg/L was analysed with an assay from Dade Behring on a BN ProSpec analyser (Siemens Healthcare Diagnostics) at Uppsala and Karolinska until 2007 and thereafter with an assay from Gentian (Gentian, Moss, Norway) on Architect ci8200 (Uppsala) and on UniCel DXC800 (Karolinska). Cystatin C was analysed with reagents from Roche on Roche Cobas c501 in Lund. The assays from Gentian and Roche were traceable to the international calibrator ERM-DA471/IFCC.8 9 All three hospital laboratories were accredited. eGFRcrea was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) creatinine equation from 2009.10 eGFRcomb was calculated using the CKD-EPI combined creatinine/cystatin C equation from 2012.6 eGFRcyst was calculated from plasma cystatin C using the international IFCC equation Caucasian, Asian, paediatric and adult cohorts (CAPA).11
Cardiovascular endpoint definition and comorbidity data
The endpoint cardiovascular mortality was defined using the International Statistical Classification of Diseases, Tenth Revision codes I00–I99, from the Swedish Cause of Death Register. I00–I99 classifies diseases of the circulatory system, including ischaemic heart diseases and cerebrovascular diseases. The registry data cover all Swedish residents and there was no loss to follow-up. Comorbidity data from 2004 and forward were collected from the Swedish National Patient Register that records data from all inpatient hospital visits in Sweden. The majority of the included patients had hospital care prior to intensive care and in those Charlson Comorbidity Index (CCI) was calculated.12 Only 3510 patients (16%) had no prior hospital care recorded in the National Patient Register. Both registers are administered by the Swedish National Board of Health and Welfare. In the process of merging the laboratory data and register data, the identity numbers were irreversibly removed and replaced by an anonymous serial number.
Statistics
The associations between eGFR (estimated with creatinine, cystatin C or a combination of them both) and cardiovascular mortality risk were analysed in Cox proportional hazard regression models. The univariate HR was computed for each 1 mL/min/1.73 m2 of eGFR from 5 to 90 using a reference point at 60 mL/min/1.73 m2 and shown as a cubic regression spline curve with knots at 20, 30 and 45 mL/min/1.73 m2. The Harrell’s C-statistics,13 95% CIs and p values were calculated using the ‘somersd’ package with the ‘lincom’ command by splitting the study population randomly into a training set and a test set. To assess the calibration of the Cox models, we used the Grønnesby and Borgan calibration test,14 within 10 risk score groups. The calibration test compares the number of events that are observed with those that are expected on the basis of estimation from the models. Further, participants were entered into the models divided in eGFR categories >60, 30–59, 20–29 and <20 mL/min/1.73 m2. The categories were according to the European Society of Cardiology clinical cardiovascular prevention guidelines for cardiovascular risk2 with the modification that 20 mL/min/1.73 m2 was used instead of the usual 15 mL/min/1.73 m2, since 20 mL/min/1.73 m2 is the clinical decision limit for continuous renal replacement therapy in the intensive care unit. Overall improvement in reclassification based on the eGFR categories >60, 30–59, 20–29 and <20 mL/min/1.73 m2 was evaluated using net reclassification improvement (NRI) according to Pencina et al.15 For reclassification analysis, the study population was first classified to an eGFR category by the creatinine and the combined equation, respectively, and the patients who reclassified to a higher or lower eGFR category by the cystatin C equation were analysed for cardiovascular mortality risk compared with the patients not reclassified using Cox proportional hazards models. Models were adjusted for age, gender and CCI since older patients, male patients and patients with a higher number of comorbidity more often reclassified to a higher eGFR risk category with cystatin C thus potentially confounded the reclassification analysis. The models were also adjusted for prior diagnosis of diabetes, obesity, hypertensive disease or previous cardiovascular disease. Calculations were performed with Stata V.16.1 (Stata Corp, College Station, Texas, USA).
Results
Baseline characteristics and cardiovascular mortality risk in the eGFR subgroups
Out of the 22 488 patients included, 10 392 (46%) patients were in a general intensive care unit, 2597 (11%) in a neurosurgical intensive care unit, 5132 (23%) in a cardiothoracic intensive care unit and 4367 (19%) in a coronary care unit. Mean (95% CI) age was 62.0 years (61.8–62.2 years) and 36% were women. The patients had a creatinine of 109 (107–110) µmol/L and cystatin C 1.34 (1.33–1.35) mg/L, corresponding to an eGFRcrea of 76.3 (75.9–76.7) mL/min/1.73 m2 and a significantly lower eGFRcyst of 73.3 (72.7–73.9) mL/min/1.73 m2. Mean CCI was 1.6 (1.5–1.6). Chronic diseases were frequent in the patient population, including cardiovascular diseases (38%), hypertension (30%), infectious diseases (25%), diabetes mellitus (16%), trauma (13%), cerebrovascular disease (11%), kidney diseases (9%), liver and biliary tract diseases (4%), obesity (2%) and intoxications (1%) as discharge diagnoses. During follow-up, 8401 (37%) participants died.
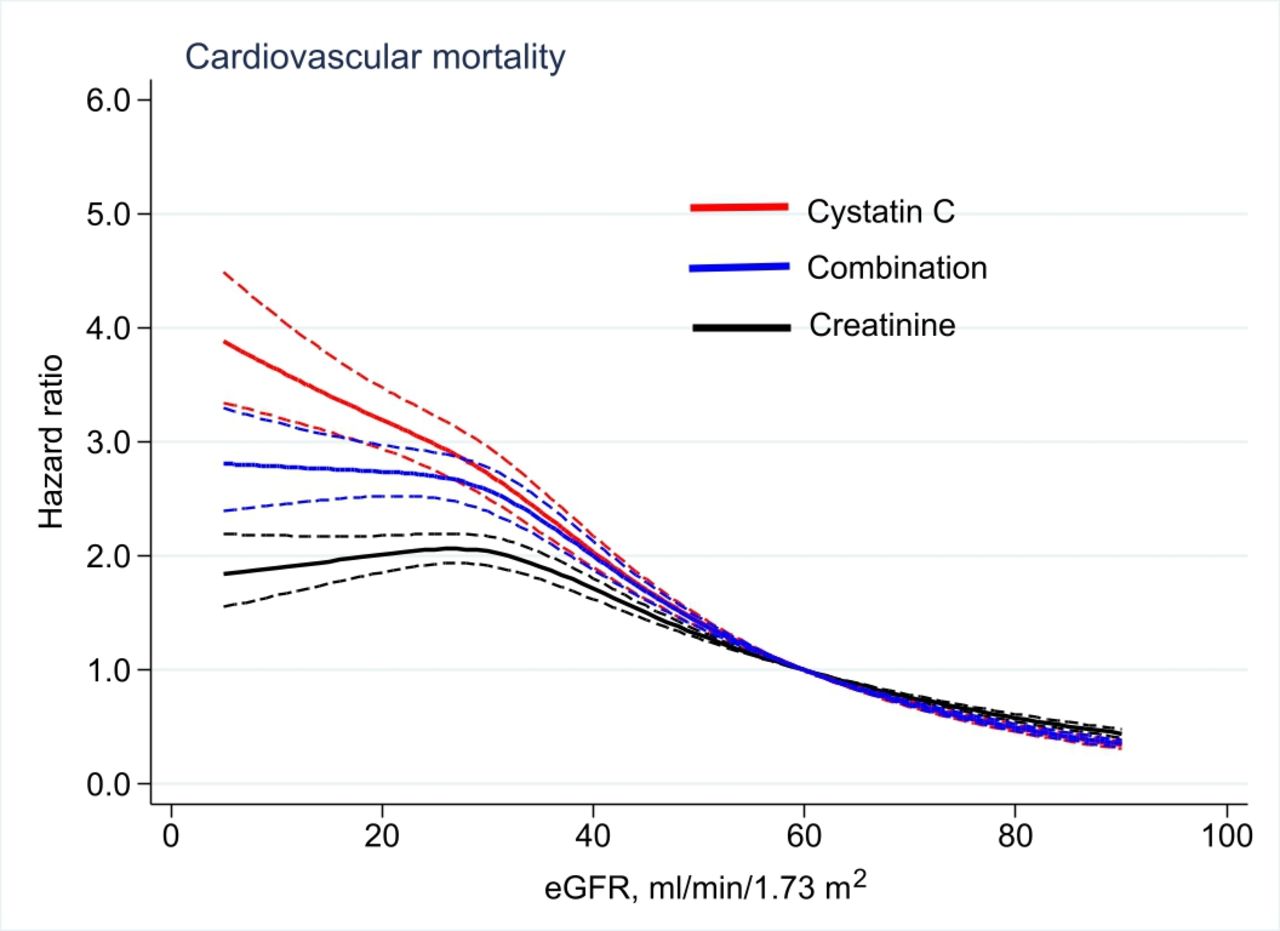
During the follow-up of 5.1 (2.3–7.1) years, median (interquartile interval), corresponding to 106 036 person-years in total, 2960 (13%) died of cardiovascular causes. Cardiovascular mortality risks in HR with 95% CIs for each equation versus the reference point at 60 mL/min/1.73 m2 are shown in figure 1 in cubic spline curves. The spline curves show that eGFR at about 50 mL/min/1.73 m2 and below, estimated with cystatin C or the combined equation, is significantly related to a higher cardiovascular mortality risk than eGFR estimated with creatinine.
{kind=link}
The HRs and 95% CIs (in thin dotted lines) for cardiovascular mortality by each equation from univariate Cox proportional hazard models are shown in cubic regression spline curves. The reference point is set to 60 mL/min/1.73 m2. eGFR, estimated glomerular filtration rate.
Incidence rates for cardiovascular mortality according to the eGFR categories >60, 30–59, 20–29 and <20 mL/min/1.73 m2, defined by respective equation, are presented in table 1. Overall, decreasing eGFR, by all equations, significantly associated with cardiovascular mortality risk, especially in the subgroup below 30 mL/min/1.73 m2 where the risk of cardiovascular death was increased five to eight times depending on eGFR equation.
Cardiovascular mortality estimates by eGFR by different equations using Cox regression; incidence rate is per 100 person-years
Harrell’s C-statistics: comparing the predictive power of eGFRcrea, eGFRcomb and eGFRcyst
For each of the eGFR equations, the predictive power was calculated with Harrell’s C-statistics (see table 2). The equations with cystatin C or the combined equation significantly increased the C-statistics for the prediction of cardiovascular death (p<0.001 vs creatinine equation). The equation with cystatin C was not superior to the combined equation (p=0.11 vs combined equation). The p values for the Grønnesby and Borgan statistics were <0.001 for all three models indicating not sufficient calibration, decile data not shown.
Harrell’s C-statistics for Cox regression models predicting cardiovascular mortality
Reclassification analysis: does eGFRcyst classify patients better than eGFRcrea with respect to cardiovascular risk?
Overall, patients reclassified to a lower GFR category by using the cystatin C-based equation, as compared with the creatinine-based equation, had significantly increased cardiovascular mortality risk (table 3) compared with the referent patients not reclassified. Contrariwise, patients reclassified to a higher GFR category by the cystatin C-based formula, as compared with the creatinine-based equation, had significantly lowered cardiovascular mortality risk. Adjustment for age, gender, CCI, and prior diagnosis of diabetes, obesity, hypertension or previous cardiovascular disease did not change the associations substantially. The calculated NRI for the cystatin C equation compared with creatinine equation was 0.15, p<0.001, indicating improved reclassification by the cystatin C equation.
Cardiovascular mortality risk when classified according to eGFR recalculated with cystatin C, as compared with creatinine
Reclassification analysis: does eGFRcyst classify patients better than eGFRcomb with respect to cardiovascular risk?
Overall, patients who reclassify to a lower GFR category by using the cystatin C-based equation, as compared with the combined equation, had significantly increased cardiovascular mortality risk (table 4) compared with the referent patients not reclassified. Contrariwise, patients who reclassify to a higher GFR category by the cystatin C-based formula, as compared with the combined equation, had a significantly lower risk for cardiovascular mortality. Adjustment for age, gender, CCI, and prior diagnosis of diabetes, obesity, hypertension or previous cardiovascular disease did not change the associations substantially. The calculated NRI for the cystatin C equation compared with combined equation was 0.04, p<0.001, indicating improved reclassification by the cystatin C equation.
Cardiovascular mortality risk when classified according to eGFR recalculated with cystatin C, as compared with the combination formula
Discussion
AKI is commonly a transitory incident in patients at intensive care. This study describes that one single cystatin C at admission to different intensive care units, alone or in combination with creatinine, predicted long-term risk of cardiovascular death better than creatinine alone. To our knowledge, this has not been described in a critically ill patient population before. However, the superiority of cystatin C in predicting cardiovascular mortality has been observed in other patient groups such as in various patients in primary health and hospital care.16 17 Further, a meta-analysis of community-based and CKD cohorts by the CKD-prognosis consortium showed that cystatin C-based eGFR equations, alone or in combination with creatinine, strengthened the association between eGFR and cardiovascular death at all different levels of kidney function.18 The underlying mechanisms for the additional value of cystatin C over creatinine alone in predicting cardiovascular death in critically ill patients are not entirely clear. It may relate to either that cystatin C has advantages as a biomarker of kidney function in the intensive care setting or possible non-GFR effects of cystatin C associated with cardiovascular disease risk or a bit of both mechanisms.
Is cystatin C a better biomarker of kidney function in critically ill patients? This theory has its origin in the well-known shortcomings of creatinine as a biomarker of GFR. The accurateness of creatinine as a GFR biomarker assumes a steady-state production, distribution and clearance of creatinine. The diet and patients’ muscle mass mainly determine the production rate of creatinine. Bedfast, critically ill, may for various reasons not be in steady state due to low meat intake and ongoing loss of muscle mass due to immobilisation, trauma or fever19 and or altered distribution volume due to fluid accumulation. As a result, these factors may potentially lead to a risk of overestimation of eGFR because of falsely low plasma creatinine values.4 7 In theory, since cystatin C is produced by all nucleated cells, freely filtered in glomeruli, not affected by malnutrition20 or loss of muscle mass,21 it may serve as an appealing alternative in estimating eGFR at least in the critically ill. Since cystatin C is produced by all nucleated cells and hence possibly falsely too high in conditions with high cell turnover such as diseases related to sepsis and inflammation. Increased C reactive protein and high leucocyte blood count, which is common in the critically ill, have been related to high cystatin C and low creatinine in observational studies.5 However, the impact of inflammation on cystatin C has been intensely discussed and studies of inflammatory responses after surgery could not confirm that cystatin C is increased as an effect of postsurgical inflammation.22 Another disadvantage of creatinine, compared with cystatin C, is slower distribution kinetics, thus it may take several days for creatinine to increase in case of kidney damage.23 In the critically ill, a timely detection of acute kidney damage is essential and cystatin C has been shown to be strongly associated with contrast-induced AKI and long-term cardiovascular and all-cause death and major cardiac adverse events.24 Nevertheless, if cystatin C is an outstanding kidney filtration biomarker in intensive care, one would expect a close relationship between gold standard measurements of GFR such as iohexol clearance. Rather, it has been shown that eGFR equations with both creatinine and cystatin C are more accurate than creatinine equations alone in the critically ill.7 This has also been reported for other patient groups such as in CKD.6
Could the added predictive value of cystatin C to long-term cardiovascular risk partly depend on other factors than true GFR? Several prospective studies show a strong relationship between cystatin C and risk of future cardiovascular events.18 25 These studies put forward the obvious link of cystatin C being a risk marker of kidney disease and thereby an important cardiovascular risk factor. However, some studies point out cystatin C as a factor related to death independent of renal function (in critically ill)3 and in patients with apparently normal kidney function,26 which supports the theory of a non-GFR-related effect of cystatin C. Cystatin C is a potent cysteine proteinase inhibitor and could theoretically influence or be influenced by the activity of the elastolytic cysteine proteases cathepsin S and K.27 Higher circulating levels of cathepsin S, which may be related to degradation of extracellular matrix and atherosclerotic plaque destabilisation, have previously been linked to increased mortality risk.28 However, a large scale Mendelian randomisation analyses, predominantly based on community-based studies, did not support a causal role of circulating cystatin C in the development of cardiovascular disease.29 Stevens et al reported that cardiovascular risk factors such as smoking, high body mass index, hyperlipidaemia and diabetes were related to cystatin C independently of measured GFR.5 Further, cystatin C has been associated with left ventricular mass, concentricity and wall thickness independently of creatinine-estimated renal function.30 In the light of these studies, it cannot be excluded that cystatin C is related to cardiovascular pathophysiology, beyond being a kidney function biomarker, and therefore linked to cardiovascular risk. However, a non-GFR linkage theory is highly speculative since most evidence here is based on cross-sectional cohort studies where causal effects are difficult to establish. It has been proposed that cystatin C might be used as a marker to identify high-risk patients with worse prognosis, thus in need of more careful follow-up.24 Additional studies are warranted to provide further insights into the underlying mechanisms of these associations and the clinical utility.
Strengths and limitations
Strengths of this study include: all biochemical analyses were performed at accredited university hospital laboratories with methods traceble to the international standard calibration, and the high quality of Swedish registry data secured no loss to follow-up. The registry data could not provide dismissal dates, thus we could unfortunately not examine the clinically important outcome in-hospital mortality versus mortality that occurred after dismissal. We are not aware of any larger study comparing creatinine and cystatin C for cardiovascular risk prediction in the critically ill and we believe that since three large university hospitals contributed with data, the generalisability to the critically ill increases. A limitation is that this study cohort lacks information of other key cardiovascular risk factors, besides kidney function, necessary for predicting cardiovascular mortality. As expected, the p values for the Grønnesby and Borgan calibration statistics were significant, indicating that the models were not sufficiently calibrated for individual risk calculation in clinical decision-making. However, the study aim was not to create an algorithm for clinical utility but to explore the additional value of cystatin C to creatinine in cardiovascular mortality prediction. Additional studies are needed to evaluate if cystatin C adds prognostic value on top of all established cardiovascular risk factors.
We were unfortunately not able to detect the cases of AKI in this study since we did not have access to the patients’ baseline creatinine before entering the critical care unit. This is a limitation since AKI is common and critical in this patient cohort and may be a possible confounding factor since creatinine may lag behind in the acute onset of kidney injury. Further, comorbidity related to cardiovascular risk (diabetes, obesity, hypertension, smoking) treated in primary care may have been missed since Swedish National Patient Register only records prior hospital care which is a disadvantage in the study. Another disadvantage is that acute organ dysfunction at admission could not be adjusted for in the models.
Conclusion
A single cystatin C at admission to the intensive care unit added predictive value to creatinine for long-term cardiovascular death risk assessment. Thus, our data favour the use of either the sole cystatin C equation or the combined cystatin C–creatinine equation when estimating GFR for risk cardiovascular risk prediction purposes in the critically ill.
Key messages
What is already known on this subject?
Loss of kidney function is a cardiovascular risk factor and predicts poor survival in critically ill patients. How kidney function should be measured for risk prediction purposes in the intensive care unit is not yet established.
What might this study add?
A single cystatin C at admission to the intensive care unit added predictive value to creatinine for long-term cardiovascular death risk assessment.
How might this impact on clinical practice?
Cystatin C, alone or in combination with creatinine, should be used for estimating glomerular filtration rate for risk prediction purposes in critically ill.
Data availability statement
The datasets generated during and/or analysed during the current study are not publicly available due to the reason that the datasets used contain information that potentially could identify individual patients. Authors are willing to share their data on reasonable request and after case-by-case assessment of such request by a local ethics committee.
Ethics statements
Patient consent for publication
Ethics approval
The Swedish Ethical Review Authority in Uppsala has reviewed and approved the study protocol (Dnr 2013/441), and the study was carried out accordingly.
References
Footnotes
Twitter @DrMaxBell
Contributors All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by JH-K, MB, BR, AD and AL. The first draft of the manuscript was written by JH-K and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.