




Athletes competing in athletics (track and field) at international level may be participating with underlying undiagnosed life-threatening cardiovascular conditions. Our objective was to analyse variations in pre-participation cardiac evaluation prevalence among athletes participating in two International Association of Athletics Federations (IAAF) World Athletics Championships, with regard to the human developmental level and global region of their home countries, as well as athletes' age category, gender, event group and medical insurance type.
Cross-sectional web-based survey.
A total of 1785 athletes competing in the IAAF World Under 18 Championships Nairobi 2017 and World Championships London 2017 were invited to complete a pre-participation health questionnaire investigating the experience of a pre-participation cardiac examination.
A total of 704 (39%) of the athletes participated. Among these, 59% (60% of women; 58% of men) reported that they had been provided at least one type of pre-participation cardiac evaluation. Athletes from very high income countries, Europe and Asia, showed a higher prevalence of at least one pre-participation cardiac evaluation.
The prevalence of pre-participation cardiac evaluation in low to middle income countries, and the African continent in particular, needs urgent attention. Furthermore, increases in evaluation prevalence should be accompanied by the development of cost-effective methods that can be adopted in all global regions.
Introduction
Athletes participating in International Association of Athletics Federations (IAAF) World Championships (WCH) represent a unique population, having reached the highest level of performance with regard to speed, power or endurance in their respective event. Nevertheless, reaching these performance levels does not exclude the underlying existence of potential life-threatening diseases,1 among which cardiovascular disorders (CVDs) could have the most dramatic consequences.2 Hereditary and congenital CVDs have been reported to be the leading causes of non-accidental death in young athletes.3,4 Several studies have shown that male athletes have a higher risk of sudden cardiac death (SCD) compared with women.5,6 The large variability reported in disease prevalence is connected to geographical differences existing among populations. The genetic background plays a significant role in the phenotypic expression of diseases that could lead to SCD.3,5 Up to date there is a lack of population-based data from low and middle-income countries (LMICs) on CVDs in the young. The high prevalence of various infectious diseases in LMICs has been suggested to modify the distribution of acquired CVDs between global regions. Africa is believed to have one of the highest prevalences of CVDs among the young, and recent studies have suggested that the burden of CVDs is underestimated in several regions mainly due to the poor outcome of children with such diseases or to the lack of infrastuctures.7 For instance, streptococcal infections, the main cause of rheumatic heart disease (RHD), are mainly found in Africa, Asia, Latin America, the Middle East and in the Pacific region.8 Given the fact that a considerable number of the athletes participating at the IAAF WCH originate from LMICs, further knowledge about athletes' cardiovascular health and cardiac evaluation history is needed.
One of the available strategies to reduce the incidence of SCD in sport is the early identification of clinically relevant CVDs through pre-participation evaluation. Therefore, the aim of this study was to analyse variations in pre-participation cardiac evaluation (PPCE) prevalence among athletes participating in IAAF WCH, with regard to the human developmental level and global region of their home countries, as well as athlete's age category, gender, event group and medical insurance type.
Methods
Study population
The national teams registered for the IAAF World Under 18 Championships Nairobi 2017 and the IAAF WCH London 2017 were considered for participation in the study. From the study population were excluded those teams that: (a) were not familiar enough with any of the available translated versions of the questionnaire (English, Spanish, Arabic, French, Portuguese, Chinese, Amharic, Russian, Japanese); (b) had to comply with their (restricted) team communication policy during championships; and/or (c) were quarantined at their hotel following Public Health England recommendations due to a norovirus outbreak (London 2017 WCH only).
Data collection
The athletes were invited personally to complete a pre-participation health questionnaire developed to collect information regarding their gender, age, country and event group (sprints, jumps, throws, middle and long-distance running, race walking and combined events). The experience of the following four cardiovascular examinations was investigated:
clinical heart examination (CHE)
12-lead rest electrocardiography (ECG)
stress ECG
trans-thoracic echocardiography examination (TTE).
The pre-participation health questionnaire was made available to athletes, as a web survey and in a paper format. The questionnaires were self-administered. Ethical approval of the study design was obtained from the research ethics board in Linköping University (Dnr. 2015/132-31).
Data analyses
Before the analysis, athletics' events were recoded into speed/power events (sprints, jumps and throws) or endurance/combined events (middle and long-distance running, including 800 m and longer, steeple chase, race walking and the combined events). The human development index (HDI) for the athlete's country of origin was used as a measure of the country's support resources.9 A summary PPCE score was built to allow composite analyses of recent cardiac evaluations that could help unmasking CVDs; CHE, 12-lead rest ECG, stress ECG and TTE were given 1 point each (score range 0 to 4).
The two variables characterising countries were recoded as below:
Developmental level of home country as defined by the United Nations (HDI) 9: low or moderate income countries (LMICs; HDI < 0.70), high income countries (HICs; 0.70 ≤ HDI < 0.80), very high income countries (VHICs; HDI ≥ 0.80).
Global region: the North American, Central American and Caribbean region (NACAC), South America, Europe, Africa, Asia, Oceania.
age category: youth (under 18 years of age) versus adult (18 years of age and older)
gender: female versus male
event-group: strength/power (throw, sprint, jump) versus endurance events (middle/long distance running, race walking, combined events)
federation health insurance (FHI): no versus yes.
The PPCE scores were first described divided by HDI category, global region, age category, gender and FHI. Comparisons of PPCE scores were performed using Mann–Whitney U tests, Kruskal–Wallis tests (with the Nemenyi test as a post-hoc test) or Spearman's rho. Differences in the prevalence of PPCE (CHE, 12-lead rest ECG, stress ECG and TTE) by HDI category and global region were first analysed using chi-squared tests (or Fisher's exact tests when motivated by underlying assumptions of data). To include athlete-level characteristics in the analyses, the distributions were thereafter analysed using log linear analysis including interactions, i.e. variable combinations. The log linear analysis started with an examination of the highest order interaction, i.e. all explanatory variables included in the analysis combined. If no differences were identified, all combinations of the next highest order interactions were examined. This procedure was continued until a statistically significant combination was found. Then, for each condition of a chosen variable in the interaction, interactions of the remaining variables were examined by separate log linear analysis. Interactions reported are those not included in any higher order interaction (except for two-way interactions described above that are reported for descriptive purposes). Only interactions including PPCE components were examined and two-way interactions were reported using chi-square statistics with odds ratios (ORs) in which odds of PPCE for each separate category was compared with odds of PPCE for all the other categories (e.g. odds for stress ECG in Europe was compared with odds for stress ECG in all the other continents).
Results
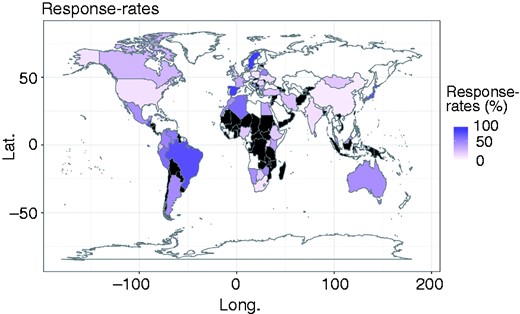
Response rates for participating countries. None-filled countries did not participate, countries in black colour had less than five eligible athletes and their response rates are not shown.
Number of participants (percentage of eligible athletes) displayed by age group (Championship), gender and global region.
| Age | Gender | NACAC | S. America | Europe | Africa | Asia | Oceania | Total |
|---|---|---|---|---|---|---|---|---|
| Youth | Women | 28 (85) | 23 (72) | 41 (25) | 52 (53) | 23 (62) | – | 167 (46) |
| Men | 30 (60) | 25 (71) | 39 (29) | 56 (46) | 23 (31) | – | 173 (42) | |
| All | 58 (70) | 48 (72) | 80 (27) | 108 (49) | 46 (41) | – | 340 (44) | |
| Adult | Women | 35 (26) | 20 (43) | 65 (42) | 27 (49) | 11 (29) | 14 (52) | 174 (38) |
| Men | 19 (12) | 33 (65) | 65 (39) | 29 (39) | 28 (43) | 13 (41) | 190 (35) | |
| All | 54 (19) | 53 (55) | 130 (41) | 56 (43) | 39 (38) | 27 (46) | 364 (36) | |
| All | Women | 63 (38) | 43 (55) | 106 (33) | 79 (52) | 34 (45) | 14 (52) | 341 (41) |
| Men | 49 (24) | 58 (67) | 104 (35) | 85 (43) | 51 (36) | 13 (41) | 363 (38) | |
| All | 112 (30) | 101 (62) | 210 (34) | 164 (47) | 85 (40) | 27 (46) | 704 (39) |
| Age | Gender | NACAC | S. America | Europe | Africa | Asia | Oceania | Total |
|---|---|---|---|---|---|---|---|---|
| Youth | Women | 28 (85) | 23 (72) | 41 (25) | 52 (53) | 23 (62) | – | 167 (46) |
| Men | 30 (60) | 25 (71) | 39 (29) | 56 (46) | 23 (31) | – | 173 (42) | |
| All | 58 (70) | 48 (72) | 80 (27) | 108 (49) | 46 (41) | – | 340 (44) | |
| Adult | Women | 35 (26) | 20 (43) | 65 (42) | 27 (49) | 11 (29) | 14 (52) | 174 (38) |
| Men | 19 (12) | 33 (65) | 65 (39) | 29 (39) | 28 (43) | 13 (41) | 190 (35) | |
| All | 54 (19) | 53 (55) | 130 (41) | 56 (43) | 39 (38) | 27 (46) | 364 (36) | |
| All | Women | 63 (38) | 43 (55) | 106 (33) | 79 (52) | 34 (45) | 14 (52) | 341 (41) |
| Men | 49 (24) | 58 (67) | 104 (35) | 85 (43) | 51 (36) | 13 (41) | 363 (38) | |
| All | 112 (30) | 101 (62) | 210 (34) | 164 (47) | 85 (40) | 27 (46) | 704 (39) |
NACAC: North American, Central American and Caribbean Athletics Association.
Youth represents participants from the Nairobi 2017 Under 18 World Championships and Adult represents participants from the London 2017 World Championships.
Number of participants (percentage of eligible athletes) displayed by age group (Championship), gender and global region.
| Age | Gender | NACAC | S. America | Europe | Africa | Asia | Oceania | Total |
|---|---|---|---|---|---|---|---|---|
| Youth | Women | 28 (85) | 23 (72) | 41 (25) | 52 (53) | 23 (62) | – | 167 (46) |
| Men | 30 (60) | 25 (71) | 39 (29) | 56 (46) | 23 (31) | – | 173 (42) | |
| All | 58 (70) | 48 (72) | 80 (27) | 108 (49) | 46 (41) | – | 340 (44) | |
| Adult | Women | 35 (26) | 20 (43) | 65 (42) | 27 (49) | 11 (29) | 14 (52) | 174 (38) |
| Men | 19 (12) | 33 (65) | 65 (39) | 29 (39) | 28 (43) | 13 (41) | 190 (35) | |
| All | 54 (19) | 53 (55) | 130 (41) | 56 (43) | 39 (38) | 27 (46) | 364 (36) | |
| All | Women | 63 (38) | 43 (55) | 106 (33) | 79 (52) | 34 (45) | 14 (52) | 341 (41) |
| Men | 49 (24) | 58 (67) | 104 (35) | 85 (43) | 51 (36) | 13 (41) | 363 (38) | |
| All | 112 (30) | 101 (62) | 210 (34) | 164 (47) | 85 (40) | 27 (46) | 704 (39) |
| Age | Gender | NACAC | S. America | Europe | Africa | Asia | Oceania | Total |
|---|---|---|---|---|---|---|---|---|
| Youth | Women | 28 (85) | 23 (72) | 41 (25) | 52 (53) | 23 (62) | – | 167 (46) |
| Men | 30 (60) | 25 (71) | 39 (29) | 56 (46) | 23 (31) | – | 173 (42) | |
| All | 58 (70) | 48 (72) | 80 (27) | 108 (49) | 46 (41) | – | 340 (44) | |
| Adult | Women | 35 (26) | 20 (43) | 65 (42) | 27 (49) | 11 (29) | 14 (52) | 174 (38) |
| Men | 19 (12) | 33 (65) | 65 (39) | 29 (39) | 28 (43) | 13 (41) | 190 (35) | |
| All | 54 (19) | 53 (55) | 130 (41) | 56 (43) | 39 (38) | 27 (46) | 364 (36) | |
| All | Women | 63 (38) | 43 (55) | 106 (33) | 79 (52) | 34 (45) | 14 (52) | 341 (41) |
| Men | 49 (24) | 58 (67) | 104 (35) | 85 (43) | 51 (36) | 13 (41) | 363 (38) | |
| All | 112 (30) | 101 (62) | 210 (34) | 164 (47) | 85 (40) | 27 (46) | 704 (39) |
NACAC: North American, Central American and Caribbean Athletics Association.
Youth represents participants from the Nairobi 2017 Under 18 World Championships and Adult represents participants from the London 2017 World Championships.
PPCE prevalence
Fifty-nine per cent of the participating athletes (60% of women; 58% of men) reported that they had been provided at least one type of PPCE (Table 2). Athletes from VHICs showed a higher prevalence of at least one PPCE (OR 4.60, 95% confidence interval (CI) 2.90–7.30) than peers from LMICs (OR 0.19, 95% CI 0.11–0.35) and HICs (OR 0.57, 95% CI 0.34–0.95; P < 0.001, ϕ = 0.25). Also, athletes from Europe (OR 4.12, 95% CI 2.48–6.84) and from Asia (OR 3.95, 95% CI 1.60–9.77) showed a higher provision of at least one PPCE, while athletes from NACAC (OR 0.28, 95% CI 0.16–0.50) and Africa (OR 0.21, 95% CI 0.12–0.38) reported a lower provision (P < 0.001, ϕ = 0.30) (Table 3). There were no general differences in reports of at least one PPCE between women and men (P = 0.757).
Number of athletes (percentage of respondents) reporting examinations displayed by development level of home country.
| LMIC | HIC | VHIC | All countries | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Youth | Adult | All | Youth | Adult | All | Youth | Adult | All | Youth | Adult | All | |
| CHE | ||||||||||||
| Power/strength | ||||||||||||
| Women | 0 (0) | 0 (0) | 0 (0) | 11 (65) | 4 (40) | 15 (56) | 2 (67) | 23 (49) | 25 (50) | 13 (57) | 27 (43) | 40 (47) |
| Men | 2 (50) | 1 (11) | 3 (23) | 2 (12) | 2 (14) | 4 (13) | 3 (100) | 23 (55) | 26 (58) | 7 (30) | 26 (40) | 33 (38) |
| Total | 2 (29) | 1 (7) | 3 (14) | 13 (39) | 6 (25) | 19 (33) | 5 (83) | 46 (52) | 51 (54) | 20 (43) | 53 (41) | 73 (42) |
| Endurance | ||||||||||||
| Women | 4 (50) | 4 (25) | 8 (33) | 3 (60) | 0 (0) | 3 (33) | 6 (100) | 22 (49) | 28 (55) | 13 (68) | 26 (40) | 39 (46) |
| Men | 1 (12) | 4 (24) | 5 (20) | 3 (38) | 2 (40) | 5 (38) | 5 (83) | 23 (57) | 28 (61) | 9 (41) | 29 (47) | 38 (45) |
| Total | 5 (31) | 8 (24) | 13 (27) | 6 (46) | 2 (22) | 8 (36) | 11 (92) | 45 (53) | 56 (58) | 22 (54) | 55 (43) | 77 (46) |
| All events | ||||||||||||
| Women | 4 (36) | 4 (18) | 8 (24) | 14 (64) | 4 (29) | 18 (50) | 8 (89) | 45 (49) | 53 (52) | 26 (62) | 53 (41) | 79 (46) |
| Men | 3 (25) | 5 (19) | 8 (21) | 5 (21) | 4 (21) | 9 (21) | 8 (89) | 46 (56) | 54 (59) | 16 (36) | 55 (43) | 71 (41) |
| Total | 7 (30) | 9 (19) | 16 (23) | 19 (41) | 8 (24) | 27 (34) | 16 (89) | 91 (52) | 107 (56) | 42 (48) | 108 (42) | 150 (44) |
| Stress ECG | ||||||||||||
| Power/strength | ||||||||||||
| Women | 0 (0) | 0 (0) | 0 (0) | 4 (27) | 3 (30) | 7 (28) | 2 (67) | 9 (19) | 11 (22) | 6 (27) | 12 (19) | 18 (21) |
| Men | 1 (25) | 1 (11) | 2 (15) | 1 (6) | 3 (21) | 4 (13) | 1 (33) | 15 (36) | 16 (36) | 3 (13) | 19 (29) | 22 (25) |
| Total | 1 (12) | 1 (7) | 2 (9) | 5 (16) | 6 (25) | 11 (20) | 3 (50) | 24 (27) | 27 (28) | 9 (20) | 31 (24) | 40 (23) |
| Endurance | ||||||||||||
| Women | 1 (12) | 0 (0) | 1 (4) | 2 (40) | 3 (75) | 5 (56) | 5 (83) | 13 (28) | 18 (35) | 8 (42) | 16 (24) | 24 (28) |
| Men | 0 (0) | 2 (12) | 2 (8) | 3 (33) | 1 (20) | 4 (29) | 4 (67) | 11 (28) | 15 (33) | 7 (30) | 14 (23) | 21 (25) |
| Total | 1 (6) | 2 (6) | 3 (6) | 5 (36) | 4 (44) | 9 (39) | 9 (75) | 24 (28) | 33 (34) | 15 (36) | 30 (24) | 45 (27) |
| All events | ||||||||||||
| Women | 1 (8) | 0 (0) | 1 (3) | 6 (30) | 6 (43) | 12 (35) | 7 (78) | 22 (24) | 29 (28) | 14 (34) | 28 (22) | 42 (25) |
| Men | 1 (8) | 3 (12) | 4 (11) | 4 (16) | 4 (21) | 8 (18) | 5 (56) | 26 (32) | 31 (34) | 10 (22) | 33 (26) | 43 (25) |
| Total | 2 (8) | 3 (6) | 5 (7) | 10 (22) | 10 (30) | 20 (26) | 12 (67) | 48 (27) | 60 (31) | 24 (28) | 61 (24) | 85 (25) |
| 12-lead rest ECG | ||||||||||||
| Power/strength | ||||||||||||
| Women | 1 (25) | 0 (0) | 1 (10) | 6 (35) | 4 (40) | 10 (37) | 3 (100) | 31 (66) | 34 (68) | 10 (42) | 35 (56) | 45 (52) |
| Men | 2 (50) | 1 (11) | 3 (23) | 4 (27) | 2 (14) | 6 (21) | 3 (100) | 31 (74) | 34 (76) | 9 (41) | 34 (52) | 43 (49) |
| Total | 3 (38) | 1 (7) | 4 (17) | 10 (31) | 6 (25) | 16 (29) | 6 (100) | 62 (70) | 68 (72) | 19 (41) | 69 (54) | 88 (51) |
| Endurance | ||||||||||||
| Women | 2 (29) | 1 (6) | 3 (13) | 3 (60) | 3 (75) | 6 (67) | 6 (100) | 26 (57) | 32 (62) | 11 (61) | 30 (45) | 41 (49) |
| Men | 2 (25) | 5 (29) | 7 (28) | 4 (44) | 1 (20) | 5 (36) | 6 (100) | 28 (70) | 34 (74) | 12 (52) | 34 (55) | 46 (54) |
| Total | 4 (27) | 6 (18) | 10 (21) | 7 (50) | 4 (44) | 11 (48) | 12(100) | 54 (63) | 66 (67) | 23 (56) | 64 (50) | 87 (51) |
| All events | ||||||||||||
| Women | 3 (27) | 1 (5) | 4 (12) | 9 (41) | 7 (50) | 16 (44) | 9 (100) | 57 (61) | 66 (65) | 21 (50) | 65 (50) | 86 (50) |
| Men | 4 (33) | 6 (23) | 10 (26) | 8 (33) | 3 (16) | 11 (26) | 9 (100) | 59 (72) | 68 (75) | 21 (47) | 68 (54) | 89 (52) |
| Total | 7 (30) | 7 (15) | 14 (20) | 17 (37) | 10 (30) | 27 (34) | 18 (100) | 116 (66) | 134 (69) | 42 (48) | 133 (52) | 175 (51) |
| Echo-cardiography | ||||||||||||
| Power/strength | ||||||||||||
| Women | 0 (0) | 0 (0) | 0 (0) | 2 (12) | 3 (30) | 5 (19) | 2 (67) | 14 (30) | 16 (33) | 4 (16) | 17 (27) | 21 (24) |
| Men | 0 (0) | 1 (11) | 1 (8) | 2 (13) | 2 (14) | 4 (14) | 1 (33) | 13 (31) | 14 (31) | 3 (14) | 16 (25) | 19 (22) |
| Total | 0 (0) | 1 (7) | 1 (4) | 4 (12) | 5 (21) | 9 (16) | 3 (50) | 27 (31) | 30 (32) | 7 (15) | 33 (26) | 40 (23) |
| Endurance | ||||||||||||
| Women | 0 (0) | 1 (6) | 1 (4) | 2 (40) | 0 (0) | 2 (22) | 3 (50) | 18 (39) | 21 (40) | 5 (28) | 19 (29) | 24 (29) |
| Men | 0 (0) | 2 (12) | 2 (8) | 3 (33) | 1 (20) | 4 (29) | 4 (67) | 13 (32) | 17 (37) | 7 (30) | 16 (26) | 23 (27) |
| Total | 0 (0) | 3 (9) | 3 (6) | 5 (36) | 1 (11) | 6 (26) | 7 (58) | 31 (36) | 38 (39) | 12 (29) | 35 (28) | 47 (28) |
| All events | ||||||||||||
| Women | 0 (0) | 1 (5) | 1 (3) | 4 (18) | 3 (21) | 7 (19) | 5 (56) | 32 (35) | 37 (37) | 9 (21) | 36 (28) | 45 (26) |
| Men | 0 (0) | 3 (12) | 3 (8) | 5 (21) | 3 (16) | 8 (19) | 5 (56) | 26 (32) | 31 (34) | 10 (22) | 32 (25) | 42 (25) |
| Total | 0 (0) | 4 (9) | 4 (6) | 9 (20) | 6 (18) | 15 (19) | 10 (56) | 58 (33) | 68 (35) | 19 (22) | 68 (27) | 87 (25) |
| At least one PPCE | ||||||||||||
| Power/strength | ||||||||||||
| Women | 1 (33) | 0 (0) | 1 (11) | 12 (71) | 4 (40) | 16 (59) | 3 (100) | 32 (70) | 35 (71) | 16 (70) | 36 (58) | 52 (61) |
| Men | 2 (50) | 2 (22) | 4 (31) | 5 (36) | 3 (21) | 8 (29) | 3 (100) | 34 (81) | 37 (82) | 10 (48) | 39 (60) | 49 (57) |
| Total | 3 (43) | 2 (13) | 5 (23) | 17 (55) | 7 (29) | 24 (44) | 6 (100) | 66 (75) | 72 (77) | 26 (59) | 75 (59) | 101 (59) |
| Endurance | ||||||||||||
| Women | 4 (50) | 4 (25) | 8 (33) | 4 (80) | 3 (75) | 7 (78) | 6 (100) | 28 (61) | 34 (65) | 14 (74) | 35 (53) | 49 (58) |
| Men | 2 (25) | 5 (29) | 7 (28) | 4 (50) | 2 (40) | 6 (46) | 6 (100) | 30 (75) | 36 (78) | 12 (55) | 37 (60) | 49 (58) |
| Total | 6 (38) | 9 (27) | 15 (31) | 8 (62) | 5 (56) | 13 (59) | 12 (100) | 58 (67) | 70 (71) | 26 (63) | 72 (56) | 98 (58) |
| All events | ||||||||||||
| Women | 5 (45) | 4 (18) | 9 (27) | 16 (73) | 7 (50) | 23 (64) | 9 (100) | 60 (65) | 69 (68) | 30 (71) | 71 (55) | 101 (59) |
| Men | 4 (33) | 7 (27) | 11 (29) | 9 (41) | 5 (26) | 14 (34) | 9 (100) | 64 (78) | 73 (80) | 22 (51) | 76 (60) | 98 (58) |
| Total | 9 (39) | 11 (23) | 20 (28) | 25 (57) | 12 (36) | 37 (48) | 18 (100) | 124 (71) | 142 (74) | 52 (61) | 147 (58) | 199 (59) |
| LMIC | HIC | VHIC | All countries | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Youth | Adult | All | Youth | Adult | All | Youth | Adult | All | Youth | Adult | All | |
| CHE | ||||||||||||
| Power/strength | ||||||||||||
| Women | 0 (0) | 0 (0) | 0 (0) | 11 (65) | 4 (40) | 15 (56) | 2 (67) | 23 (49) | 25 (50) | 13 (57) | 27 (43) | 40 (47) |
| Men | 2 (50) | 1 (11) | 3 (23) | 2 (12) | 2 (14) | 4 (13) | 3 (100) | 23 (55) | 26 (58) | 7 (30) | 26 (40) | 33 (38) |
| Total | 2 (29) | 1 (7) | 3 (14) | 13 (39) | 6 (25) | 19 (33) | 5 (83) | 46 (52) | 51 (54) | 20 (43) | 53 (41) | 73 (42) |
| Endurance | ||||||||||||
| Women | 4 (50) | 4 (25) | 8 (33) | 3 (60) | 0 (0) | 3 (33) | 6 (100) | 22 (49) | 28 (55) | 13 (68) | 26 (40) | 39 (46) |
| Men | 1 (12) | 4 (24) | 5 (20) | 3 (38) | 2 (40) | 5 (38) | 5 (83) | 23 (57) | 28 (61) | 9 (41) | 29 (47) | 38 (45) |
| Total | 5 (31) | 8 (24) | 13 (27) | 6 (46) | 2 (22) | 8 (36) | 11 (92) | 45 (53) | 56 (58) | 22 (54) | 55 (43) | 77 (46) |
| All events | ||||||||||||
| Women | 4 (36) | 4 (18) | 8 (24) | 14 (64) | 4 (29) | 18 (50) | 8 (89) | 45 (49) | 53 (52) | 26 (62) | 53 (41) | 79 (46) |
| Men | 3 (25) | 5 (19) | 8 (21) | 5 (21) | 4 (21) | 9 (21) | 8 (89) | 46 (56) | 54 (59) | 16 (36) | 55 (43) | 71 (41) |
| Total | 7 (30) | 9 (19) | 16 (23) | 19 (41) | 8 (24) | 27 (34) | 16 (89) | 91 (52) | 107 (56) | 42 (48) | 108 (42) | 150 (44) |
| Stress ECG | ||||||||||||
| Power/strength | ||||||||||||
| Women | 0 (0) | 0 (0) | 0 (0) | 4 (27) | 3 (30) | 7 (28) | 2 (67) | 9 (19) | 11 (22) | 6 (27) | 12 (19) | 18 (21) |
| Men | 1 (25) | 1 (11) | 2 (15) | 1 (6) | 3 (21) | 4 (13) | 1 (33) | 15 (36) | 16 (36) | 3 (13) | 19 (29) | 22 (25) |
| Total | 1 (12) | 1 (7) | 2 (9) | 5 (16) | 6 (25) | 11 (20) | 3 (50) | 24 (27) | 27 (28) | 9 (20) | 31 (24) | 40 (23) |
| Endurance | ||||||||||||
| Women | 1 (12) | 0 (0) | 1 (4) | 2 (40) | 3 (75) | 5 (56) | 5 (83) | 13 (28) | 18 (35) | 8 (42) | 16 (24) | 24 (28) |
| Men | 0 (0) | 2 (12) | 2 (8) | 3 (33) | 1 (20) | 4 (29) | 4 (67) | 11 (28) | 15 (33) | 7 (30) | 14 (23) | 21 (25) |
| Total | 1 (6) | 2 (6) | 3 (6) | 5 (36) | 4 (44) | 9 (39) | 9 (75) | 24 (28) | 33 (34) | 15 (36) | 30 (24) | 45 (27) |
| All events | ||||||||||||
| Women | 1 (8) | 0 (0) | 1 (3) | 6 (30) | 6 (43) | 12 (35) | 7 (78) | 22 (24) | 29 (28) | 14 (34) | 28 (22) | 42 (25) |
| Men | 1 (8) | 3 (12) | 4 (11) | 4 (16) | 4 (21) | 8 (18) | 5 (56) | 26 (32) | 31 (34) | 10 (22) | 33 (26) | 43 (25) |
| Total | 2 (8) | 3 (6) | 5 (7) | 10 (22) | 10 (30) | 20 (26) | 12 (67) | 48 (27) | 60 (31) | 24 (28) | 61 (24) | 85 (25) |
| 12-lead rest ECG | ||||||||||||
| Power/strength | ||||||||||||
| Women | 1 (25) | 0 (0) | 1 (10) | 6 (35) | 4 (40) | 10 (37) | 3 (100) | 31 (66) | 34 (68) | 10 (42) | 35 (56) | 45 (52) |
| Men | 2 (50) | 1 (11) | 3 (23) | 4 (27) | 2 (14) | 6 (21) | 3 (100) | 31 (74) | 34 (76) | 9 (41) | 34 (52) | 43 (49) |
| Total | 3 (38) | 1 (7) | 4 (17) | 10 (31) | 6 (25) | 16 (29) | 6 (100) | 62 (70) | 68 (72) | 19 (41) | 69 (54) | 88 (51) |
| Endurance | ||||||||||||
| Women | 2 (29) | 1 (6) | 3 (13) | 3 (60) | 3 (75) | 6 (67) | 6 (100) | 26 (57) | 32 (62) | 11 (61) | 30 (45) | 41 (49) |
| Men | 2 (25) | 5 (29) | 7 (28) | 4 (44) | 1 (20) | 5 (36) | 6 (100) | 28 (70) | 34 (74) | 12 (52) | 34 (55) | 46 (54) |
| Total | 4 (27) | 6 (18) | 10 (21) | 7 (50) | 4 (44) | 11 (48) | 12(100) | 54 (63) | 66 (67) | 23 (56) | 64 (50) | 87 (51) |
| All events | ||||||||||||
| Women | 3 (27) | 1 (5) | 4 (12) | 9 (41) | 7 (50) | 16 (44) | 9 (100) | 57 (61) | 66 (65) | 21 (50) | 65 (50) | 86 (50) |
| Men | 4 (33) | 6 (23) | 10 (26) | 8 (33) | 3 (16) | 11 (26) | 9 (100) | 59 (72) | 68 (75) | 21 (47) | 68 (54) | 89 (52) |
| Total | 7 (30) | 7 (15) | 14 (20) | 17 (37) | 10 (30) | 27 (34) | 18 (100) | 116 (66) | 134 (69) | 42 (48) | 133 (52) | 175 (51) |
| Echo-cardiography | ||||||||||||
| Power/strength | ||||||||||||
| Women | 0 (0) | 0 (0) | 0 (0) | 2 (12) | 3 (30) | 5 (19) | 2 (67) | 14 (30) | 16 (33) | 4 (16) | 17 (27) | 21 (24) |
| Men | 0 (0) | 1 (11) | 1 (8) | 2 (13) | 2 (14) | 4 (14) | 1 (33) | 13 (31) | 14 (31) | 3 (14) | 16 (25) | 19 (22) |
| Total | 0 (0) | 1 (7) | 1 (4) | 4 (12) | 5 (21) | 9 (16) | 3 (50) | 27 (31) | 30 (32) | 7 (15) | 33 (26) | 40 (23) |
| Endurance | ||||||||||||
| Women | 0 (0) | 1 (6) | 1 (4) | 2 (40) | 0 (0) | 2 (22) | 3 (50) | 18 (39) | 21 (40) | 5 (28) | 19 (29) | 24 (29) |
| Men | 0 (0) | 2 (12) | 2 (8) | 3 (33) | 1 (20) | 4 (29) | 4 (67) | 13 (32) | 17 (37) | 7 (30) | 16 (26) | 23 (27) |
| Total | 0 (0) | 3 (9) | 3 (6) | 5 (36) | 1 (11) | 6 (26) | 7 (58) | 31 (36) | 38 (39) | 12 (29) | 35 (28) | 47 (28) |
| All events | ||||||||||||
| Women | 0 (0) | 1 (5) | 1 (3) | 4 (18) | 3 (21) | 7 (19) | 5 (56) | 32 (35) | 37 (37) | 9 (21) | 36 (28) | 45 (26) |
| Men | 0 (0) | 3 (12) | 3 (8) | 5 (21) | 3 (16) | 8 (19) | 5 (56) | 26 (32) | 31 (34) | 10 (22) | 32 (25) | 42 (25) |
| Total | 0 (0) | 4 (9) | 4 (6) | 9 (20) | 6 (18) | 15 (19) | 10 (56) | 58 (33) | 68 (35) | 19 (22) | 68 (27) | 87 (25) |
| At least one PPCE | ||||||||||||
| Power/strength | ||||||||||||
| Women | 1 (33) | 0 (0) | 1 (11) | 12 (71) | 4 (40) | 16 (59) | 3 (100) | 32 (70) | 35 (71) | 16 (70) | 36 (58) | 52 (61) |
| Men | 2 (50) | 2 (22) | 4 (31) | 5 (36) | 3 (21) | 8 (29) | 3 (100) | 34 (81) | 37 (82) | 10 (48) | 39 (60) | 49 (57) |
| Total | 3 (43) | 2 (13) | 5 (23) | 17 (55) | 7 (29) | 24 (44) | 6 (100) | 66 (75) | 72 (77) | 26 (59) | 75 (59) | 101 (59) |
| Endurance | ||||||||||||
| Women | 4 (50) | 4 (25) | 8 (33) | 4 (80) | 3 (75) | 7 (78) | 6 (100) | 28 (61) | 34 (65) | 14 (74) | 35 (53) | 49 (58) |
| Men | 2 (25) | 5 (29) | 7 (28) | 4 (50) | 2 (40) | 6 (46) | 6 (100) | 30 (75) | 36 (78) | 12 (55) | 37 (60) | 49 (58) |
| Total | 6 (38) | 9 (27) | 15 (31) | 8 (62) | 5 (56) | 13 (59) | 12 (100) | 58 (67) | 70 (71) | 26 (63) | 72 (56) | 98 (58) |
| All events | ||||||||||||
| Women | 5 (45) | 4 (18) | 9 (27) | 16 (73) | 7 (50) | 23 (64) | 9 (100) | 60 (65) | 69 (68) | 30 (71) | 71 (55) | 101 (59) |
| Men | 4 (33) | 7 (27) | 11 (29) | 9 (41) | 5 (26) | 14 (34) | 9 (100) | 64 (78) | 73 (80) | 22 (51) | 76 (60) | 98 (58) |
| Total | 9 (39) | 11 (23) | 20 (28) | 25 (57) | 12 (36) | 37 (48) | 18 (100) | 124 (71) | 142 (74) | 52 (61) | 147 (58) | 199 (59) |
LMIC: low or moderate level of human development index (HDI); HIC: high level of HDI; VHIC: very high level of HDI.
Age category (youth vs. adult), event type (power/strength, endurance) and gender (women, men).
Examinations were clinical heart examination (CHE), 12-lead electrocardiogram (12-lead rest ECG), stress electrocardiogram (stress ECG), echocardiography examination and at least one Pre-participation cardiac evaluation (PPCE).
Number of athletes (percentage of respondents) reporting examinations displayed by development level of home country.
| LMIC | HIC | VHIC | All countries | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Youth | Adult | All | Youth | Adult | All | Youth | Adult | All | Youth | Adult | All | |
| CHE | ||||||||||||
| Power/strength | ||||||||||||
| Women | 0 (0) | 0 (0) | 0 (0) | 11 (65) | 4 (40) | 15 (56) | 2 (67) | 23 (49) | 25 (50) | 13 (57) | 27 (43) | 40 (47) |
| Men | 2 (50) | 1 (11) | 3 (23) | 2 (12) | 2 (14) | 4 (13) | 3 (100) | 23 (55) | 26 (58) | 7 (30) | 26 (40) | 33 (38) |
| Total | 2 (29) | 1 (7) | 3 (14) | 13 (39) | 6 (25) | 19 (33) | 5 (83) | 46 (52) | 51 (54) | 20 (43) | 53 (41) | 73 (42) |
| Endurance | ||||||||||||
| Women | 4 (50) | 4 (25) | 8 (33) | 3 (60) | 0 (0) | 3 (33) | 6 (100) | 22 (49) | 28 (55) | 13 (68) | 26 (40) | 39 (46) |
| Men | 1 (12) | 4 (24) | 5 (20) | 3 (38) | 2 (40) | 5 (38) | 5 (83) | 23 (57) | 28 (61) | 9 (41) | 29 (47) | 38 (45) |
| Total | 5 (31) | 8 (24) | 13 (27) | 6 (46) | 2 (22) | 8 (36) | 11 (92) | 45 (53) | 56 (58) | 22 (54) | 55 (43) | 77 (46) |
| All events | ||||||||||||
| Women | 4 (36) | 4 (18) | 8 (24) | 14 (64) | 4 (29) | 18 (50) | 8 (89) | 45 (49) | 53 (52) | 26 (62) | 53 (41) | 79 (46) |
| Men | 3 (25) | 5 (19) | 8 (21) | 5 (21) | 4 (21) | 9 (21) | 8 (89) | 46 (56) | 54 (59) | 16 (36) | 55 (43) | 71 (41) |
| Total | 7 (30) | 9 (19) | 16 (23) | 19 (41) | 8 (24) | 27 (34) | 16 (89) | 91 (52) | 107 (56) | 42 (48) | 108 (42) | 150 (44) |
| Stress ECG | ||||||||||||
| Power/strength | ||||||||||||
| Women | 0 (0) | 0 (0) | 0 (0) | 4 (27) | 3 (30) | 7 (28) | 2 (67) | 9 (19) | 11 (22) | 6 (27) | 12 (19) | 18 (21) |
| Men | 1 (25) | 1 (11) | 2 (15) | 1 (6) | 3 (21) | 4 (13) | 1 (33) | 15 (36) | 16 (36) | 3 (13) | 19 (29) | 22 (25) |
| Total | 1 (12) | 1 (7) | 2 (9) | 5 (16) | 6 (25) | 11 (20) | 3 (50) | 24 (27) | 27 (28) | 9 (20) | 31 (24) | 40 (23) |
| Endurance | ||||||||||||
| Women | 1 (12) | 0 (0) | 1 (4) | 2 (40) | 3 (75) | 5 (56) | 5 (83) | 13 (28) | 18 (35) | 8 (42) | 16 (24) | 24 (28) |
| Men | 0 (0) | 2 (12) | 2 (8) | 3 (33) | 1 (20) | 4 (29) | 4 (67) | 11 (28) | 15 (33) | 7 (30) | 14 (23) | 21 (25) |
| Total | 1 (6) | 2 (6) | 3 (6) | 5 (36) | 4 (44) | 9 (39) | 9 (75) | 24 (28) | 33 (34) | 15 (36) | 30 (24) | 45 (27) |
| All events | ||||||||||||
| Women | 1 (8) | 0 (0) | 1 (3) | 6 (30) | 6 (43) | 12 (35) | 7 (78) | 22 (24) | 29 (28) | 14 (34) | 28 (22) | 42 (25) |
| Men | 1 (8) | 3 (12) | 4 (11) | 4 (16) | 4 (21) | 8 (18) | 5 (56) | 26 (32) | 31 (34) | 10 (22) | 33 (26) | 43 (25) |
| Total | 2 (8) | 3 (6) | 5 (7) | 10 (22) | 10 (30) | 20 (26) | 12 (67) | 48 (27) | 60 (31) | 24 (28) | 61 (24) | 85 (25) |
| 12-lead rest ECG | ||||||||||||
| Power/strength | ||||||||||||
| Women | 1 (25) | 0 (0) | 1 (10) | 6 (35) | 4 (40) | 10 (37) | 3 (100) | 31 (66) | 34 (68) | 10 (42) | 35 (56) | 45 (52) |
| Men | 2 (50) | 1 (11) | 3 (23) | 4 (27) | 2 (14) | 6 (21) | 3 (100) | 31 (74) | 34 (76) | 9 (41) | 34 (52) | 43 (49) |
| Total | 3 (38) | 1 (7) | 4 (17) | 10 (31) | 6 (25) | 16 (29) | 6 (100) | 62 (70) | 68 (72) | 19 (41) | 69 (54) | 88 (51) |
| Endurance | ||||||||||||
| Women | 2 (29) | 1 (6) | 3 (13) | 3 (60) | 3 (75) | 6 (67) | 6 (100) | 26 (57) | 32 (62) | 11 (61) | 30 (45) | 41 (49) |
| Men | 2 (25) | 5 (29) | 7 (28) | 4 (44) | 1 (20) | 5 (36) | 6 (100) | 28 (70) | 34 (74) | 12 (52) | 34 (55) | 46 (54) |
| Total | 4 (27) | 6 (18) | 10 (21) | 7 (50) | 4 (44) | 11 (48) | 12(100) | 54 (63) | 66 (67) | 23 (56) | 64 (50) | 87 (51) |
| All events | ||||||||||||
| Women | 3 (27) | 1 (5) | 4 (12) | 9 (41) | 7 (50) | 16 (44) | 9 (100) | 57 (61) | 66 (65) | 21 (50) | 65 (50) | 86 (50) |
| Men | 4 (33) | 6 (23) | 10 (26) | 8 (33) | 3 (16) | 11 (26) | 9 (100) | 59 (72) | 68 (75) | 21 (47) | 68 (54) | 89 (52) |
| Total | 7 (30) | 7 (15) | 14 (20) | 17 (37) | 10 (30) | 27 (34) | 18 (100) | 116 (66) | 134 (69) | 42 (48) | 133 (52) | 175 (51) |
| Echo-cardiography | ||||||||||||
| Power/strength | ||||||||||||
| Women | 0 (0) | 0 (0) | 0 (0) | 2 (12) | 3 (30) | 5 (19) | 2 (67) | 14 (30) | 16 (33) | 4 (16) | 17 (27) | 21 (24) |
| Men | 0 (0) | 1 (11) | 1 (8) | 2 (13) | 2 (14) | 4 (14) | 1 (33) | 13 (31) | 14 (31) | 3 (14) | 16 (25) | 19 (22) |
| Total | 0 (0) | 1 (7) | 1 (4) | 4 (12) | 5 (21) | 9 (16) | 3 (50) | 27 (31) | 30 (32) | 7 (15) | 33 (26) | 40 (23) |
| Endurance | ||||||||||||
| Women | 0 (0) | 1 (6) | 1 (4) | 2 (40) | 0 (0) | 2 (22) | 3 (50) | 18 (39) | 21 (40) | 5 (28) | 19 (29) | 24 (29) |
| Men | 0 (0) | 2 (12) | 2 (8) | 3 (33) | 1 (20) | 4 (29) | 4 (67) | 13 (32) | 17 (37) | 7 (30) | 16 (26) | 23 (27) |
| Total | 0 (0) | 3 (9) | 3 (6) | 5 (36) | 1 (11) | 6 (26) | 7 (58) | 31 (36) | 38 (39) | 12 (29) | 35 (28) | 47 (28) |
| All events | ||||||||||||
| Women | 0 (0) | 1 (5) | 1 (3) | 4 (18) | 3 (21) | 7 (19) | 5 (56) | 32 (35) | 37 (37) | 9 (21) | 36 (28) | 45 (26) |
| Men | 0 (0) | 3 (12) | 3 (8) | 5 (21) | 3 (16) | 8 (19) | 5 (56) | 26 (32) | 31 (34) | 10 (22) | 32 (25) | 42 (25) |
| Total | 0 (0) | 4 (9) | 4 (6) | 9 (20) | 6 (18) | 15 (19) | 10 (56) | 58 (33) | 68 (35) | 19 (22) | 68 (27) | 87 (25) |
| At least one PPCE | ||||||||||||
| Power/strength | ||||||||||||
| Women | 1 (33) | 0 (0) | 1 (11) | 12 (71) | 4 (40) | 16 (59) | 3 (100) | 32 (70) | 35 (71) | 16 (70) | 36 (58) | 52 (61) |
| Men | 2 (50) | 2 (22) | 4 (31) | 5 (36) | 3 (21) | 8 (29) | 3 (100) | 34 (81) | 37 (82) | 10 (48) | 39 (60) | 49 (57) |
| Total | 3 (43) | 2 (13) | 5 (23) | 17 (55) | 7 (29) | 24 (44) | 6 (100) | 66 (75) | 72 (77) | 26 (59) | 75 (59) | 101 (59) |
| Endurance | ||||||||||||
| Women | 4 (50) | 4 (25) | 8 (33) | 4 (80) | 3 (75) | 7 (78) | 6 (100) | 28 (61) | 34 (65) | 14 (74) | 35 (53) | 49 (58) |
| Men | 2 (25) | 5 (29) | 7 (28) | 4 (50) | 2 (40) | 6 (46) | 6 (100) | 30 (75) | 36 (78) | 12 (55) | 37 (60) | 49 (58) |
| Total | 6 (38) | 9 (27) | 15 (31) | 8 (62) | 5 (56) | 13 (59) | 12 (100) | 58 (67) | 70 (71) | 26 (63) | 72 (56) | 98 (58) |
| All events | ||||||||||||
| Women | 5 (45) | 4 (18) | 9 (27) | 16 (73) | 7 (50) | 23 (64) | 9 (100) | 60 (65) | 69 (68) | 30 (71) | 71 (55) | 101 (59) |
| Men | 4 (33) | 7 (27) | 11 (29) | 9 (41) | 5 (26) | 14 (34) | 9 (100) | 64 (78) | 73 (80) | 22 (51) | 76 (60) | 98 (58) |
| Total | 9 (39) | 11 (23) | 20 (28) | 25 (57) | 12 (36) | 37 (48) | 18 (100) | 124 (71) | 142 (74) | 52 (61) | 147 (58) | 199 (59) |
| LMIC | HIC | VHIC | All countries | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Youth | Adult | All | Youth | Adult | All | Youth | Adult | All | Youth | Adult | All | |
| CHE | ||||||||||||
| Power/strength | ||||||||||||
| Women | 0 (0) | 0 (0) | 0 (0) | 11 (65) | 4 (40) | 15 (56) | 2 (67) | 23 (49) | 25 (50) | 13 (57) | 27 (43) | 40 (47) |
| Men | 2 (50) | 1 (11) | 3 (23) | 2 (12) | 2 (14) | 4 (13) | 3 (100) | 23 (55) | 26 (58) | 7 (30) | 26 (40) | 33 (38) |
| Total | 2 (29) | 1 (7) | 3 (14) | 13 (39) | 6 (25) | 19 (33) | 5 (83) | 46 (52) | 51 (54) | 20 (43) | 53 (41) | 73 (42) |
| Endurance | ||||||||||||
| Women | 4 (50) | 4 (25) | 8 (33) | 3 (60) | 0 (0) | 3 (33) | 6 (100) | 22 (49) | 28 (55) | 13 (68) | 26 (40) | 39 (46) |
| Men | 1 (12) | 4 (24) | 5 (20) | 3 (38) | 2 (40) | 5 (38) | 5 (83) | 23 (57) | 28 (61) | 9 (41) | 29 (47) | 38 (45) |
| Total | 5 (31) | 8 (24) | 13 (27) | 6 (46) | 2 (22) | 8 (36) | 11 (92) | 45 (53) | 56 (58) | 22 (54) | 55 (43) | 77 (46) |
| All events | ||||||||||||
| Women | 4 (36) | 4 (18) | 8 (24) | 14 (64) | 4 (29) | 18 (50) | 8 (89) | 45 (49) | 53 (52) | 26 (62) | 53 (41) | 79 (46) |
| Men | 3 (25) | 5 (19) | 8 (21) | 5 (21) | 4 (21) | 9 (21) | 8 (89) | 46 (56) | 54 (59) | 16 (36) | 55 (43) | 71 (41) |
| Total | 7 (30) | 9 (19) | 16 (23) | 19 (41) | 8 (24) | 27 (34) | 16 (89) | 91 (52) | 107 (56) | 42 (48) | 108 (42) | 150 (44) |
| Stress ECG | ||||||||||||
| Power/strength | ||||||||||||
| Women | 0 (0) | 0 (0) | 0 (0) | 4 (27) | 3 (30) | 7 (28) | 2 (67) | 9 (19) | 11 (22) | 6 (27) | 12 (19) | 18 (21) |
| Men | 1 (25) | 1 (11) | 2 (15) | 1 (6) | 3 (21) | 4 (13) | 1 (33) | 15 (36) | 16 (36) | 3 (13) | 19 (29) | 22 (25) |
| Total | 1 (12) | 1 (7) | 2 (9) | 5 (16) | 6 (25) | 11 (20) | 3 (50) | 24 (27) | 27 (28) | 9 (20) | 31 (24) | 40 (23) |
| Endurance | ||||||||||||
| Women | 1 (12) | 0 (0) | 1 (4) | 2 (40) | 3 (75) | 5 (56) | 5 (83) | 13 (28) | 18 (35) | 8 (42) | 16 (24) | 24 (28) |
| Men | 0 (0) | 2 (12) | 2 (8) | 3 (33) | 1 (20) | 4 (29) | 4 (67) | 11 (28) | 15 (33) | 7 (30) | 14 (23) | 21 (25) |
| Total | 1 (6) | 2 (6) | 3 (6) | 5 (36) | 4 (44) | 9 (39) | 9 (75) | 24 (28) | 33 (34) | 15 (36) | 30 (24) | 45 (27) |
| All events | ||||||||||||
| Women | 1 (8) | 0 (0) | 1 (3) | 6 (30) | 6 (43) | 12 (35) | 7 (78) | 22 (24) | 29 (28) | 14 (34) | 28 (22) | 42 (25) |
| Men | 1 (8) | 3 (12) | 4 (11) | 4 (16) | 4 (21) | 8 (18) | 5 (56) | 26 (32) | 31 (34) | 10 (22) | 33 (26) | 43 (25) |
| Total | 2 (8) | 3 (6) | 5 (7) | 10 (22) | 10 (30) | 20 (26) | 12 (67) | 48 (27) | 60 (31) | 24 (28) | 61 (24) | 85 (25) |
| 12-lead rest ECG | ||||||||||||
| Power/strength | ||||||||||||
| Women | 1 (25) | 0 (0) | 1 (10) | 6 (35) | 4 (40) | 10 (37) | 3 (100) | 31 (66) | 34 (68) | 10 (42) | 35 (56) | 45 (52) |
| Men | 2 (50) | 1 (11) | 3 (23) | 4 (27) | 2 (14) | 6 (21) | 3 (100) | 31 (74) | 34 (76) | 9 (41) | 34 (52) | 43 (49) |
| Total | 3 (38) | 1 (7) | 4 (17) | 10 (31) | 6 (25) | 16 (29) | 6 (100) | 62 (70) | 68 (72) | 19 (41) | 69 (54) | 88 (51) |
| Endurance | ||||||||||||
| Women | 2 (29) | 1 (6) | 3 (13) | 3 (60) | 3 (75) | 6 (67) | 6 (100) | 26 (57) | 32 (62) | 11 (61) | 30 (45) | 41 (49) |
| Men | 2 (25) | 5 (29) | 7 (28) | 4 (44) | 1 (20) | 5 (36) | 6 (100) | 28 (70) | 34 (74) | 12 (52) | 34 (55) | 46 (54) |
| Total | 4 (27) | 6 (18) | 10 (21) | 7 (50) | 4 (44) | 11 (48) | 12(100) | 54 (63) | 66 (67) | 23 (56) | 64 (50) | 87 (51) |
| All events | ||||||||||||
| Women | 3 (27) | 1 (5) | 4 (12) | 9 (41) | 7 (50) | 16 (44) | 9 (100) | 57 (61) | 66 (65) | 21 (50) | 65 (50) | 86 (50) |
| Men | 4 (33) | 6 (23) | 10 (26) | 8 (33) | 3 (16) | 11 (26) | 9 (100) | 59 (72) | 68 (75) | 21 (47) | 68 (54) | 89 (52) |
| Total | 7 (30) | 7 (15) | 14 (20) | 17 (37) | 10 (30) | 27 (34) | 18 (100) | 116 (66) | 134 (69) | 42 (48) | 133 (52) | 175 (51) |
| Echo-cardiography | ||||||||||||
| Power/strength | ||||||||||||
| Women | 0 (0) | 0 (0) | 0 (0) | 2 (12) | 3 (30) | 5 (19) | 2 (67) | 14 (30) | 16 (33) | 4 (16) | 17 (27) | 21 (24) |
| Men | 0 (0) | 1 (11) | 1 (8) | 2 (13) | 2 (14) | 4 (14) | 1 (33) | 13 (31) | 14 (31) | 3 (14) | 16 (25) | 19 (22) |
| Total | 0 (0) | 1 (7) | 1 (4) | 4 (12) | 5 (21) | 9 (16) | 3 (50) | 27 (31) | 30 (32) | 7 (15) | 33 (26) | 40 (23) |
| Endurance | ||||||||||||
| Women | 0 (0) | 1 (6) | 1 (4) | 2 (40) | 0 (0) | 2 (22) | 3 (50) | 18 (39) | 21 (40) | 5 (28) | 19 (29) | 24 (29) |
| Men | 0 (0) | 2 (12) | 2 (8) | 3 (33) | 1 (20) | 4 (29) | 4 (67) | 13 (32) | 17 (37) | 7 (30) | 16 (26) | 23 (27) |
| Total | 0 (0) | 3 (9) | 3 (6) | 5 (36) | 1 (11) | 6 (26) | 7 (58) | 31 (36) | 38 (39) | 12 (29) | 35 (28) | 47 (28) |
| All events | ||||||||||||
| Women | 0 (0) | 1 (5) | 1 (3) | 4 (18) | 3 (21) | 7 (19) | 5 (56) | 32 (35) | 37 (37) | 9 (21) | 36 (28) | 45 (26) |
| Men | 0 (0) | 3 (12) | 3 (8) | 5 (21) | 3 (16) | 8 (19) | 5 (56) | 26 (32) | 31 (34) | 10 (22) | 32 (25) | 42 (25) |
| Total | 0 (0) | 4 (9) | 4 (6) | 9 (20) | 6 (18) | 15 (19) | 10 (56) | 58 (33) | 68 (35) | 19 (22) | 68 (27) | 87 (25) |
| At least one PPCE | ||||||||||||
| Power/strength | ||||||||||||
| Women | 1 (33) | 0 (0) | 1 (11) | 12 (71) | 4 (40) | 16 (59) | 3 (100) | 32 (70) | 35 (71) | 16 (70) | 36 (58) | 52 (61) |
| Men | 2 (50) | 2 (22) | 4 (31) | 5 (36) | 3 (21) | 8 (29) | 3 (100) | 34 (81) | 37 (82) | 10 (48) | 39 (60) | 49 (57) |
| Total | 3 (43) | 2 (13) | 5 (23) | 17 (55) | 7 (29) | 24 (44) | 6 (100) | 66 (75) | 72 (77) | 26 (59) | 75 (59) | 101 (59) |
| Endurance | ||||||||||||
| Women | 4 (50) | 4 (25) | 8 (33) | 4 (80) | 3 (75) | 7 (78) | 6 (100) | 28 (61) | 34 (65) | 14 (74) | 35 (53) | 49 (58) |
| Men | 2 (25) | 5 (29) | 7 (28) | 4 (50) | 2 (40) | 6 (46) | 6 (100) | 30 (75) | 36 (78) | 12 (55) | 37 (60) | 49 (58) |
| Total | 6 (38) | 9 (27) | 15 (31) | 8 (62) | 5 (56) | 13 (59) | 12 (100) | 58 (67) | 70 (71) | 26 (63) | 72 (56) | 98 (58) |
| All events | ||||||||||||
| Women | 5 (45) | 4 (18) | 9 (27) | 16 (73) | 7 (50) | 23 (64) | 9 (100) | 60 (65) | 69 (68) | 30 (71) | 71 (55) | 101 (59) |
| Men | 4 (33) | 7 (27) | 11 (29) | 9 (41) | 5 (26) | 14 (34) | 9 (100) | 64 (78) | 73 (80) | 22 (51) | 76 (60) | 98 (58) |
| Total | 9 (39) | 11 (23) | 20 (28) | 25 (57) | 12 (36) | 37 (48) | 18 (100) | 124 (71) | 142 (74) | 52 (61) | 147 (58) | 199 (59) |
LMIC: low or moderate level of human development index (HDI); HIC: high level of HDI; VHIC: very high level of HDI.
Age category (youth vs. adult), event type (power/strength, endurance) and gender (women, men).
Examinations were clinical heart examination (CHE), 12-lead electrocardiogram (12-lead rest ECG), stress electrocardiogram (stress ECG), echocardiography examination and at least one Pre-participation cardiac evaluation (PPCE).
Number of athletes (percentage of respondents) reporting examinations displayed by continent, event type (power/strength, endurance) and gender (women, men).
| NACAC | S. America | Europe | Africa | Asia | Oceania | All | |
|---|---|---|---|---|---|---|---|
| CHE | |||||||
| Power/strength | |||||||
| Women | 7 (28) | 6 (75) | 22 (65) | 0 (0) | 4 (67) | 2 (33) | 41 (47) |
| Men | 0 (0) | 3 (25) | 19 (63) | 4 (36) | 6 (43) | 1 (20) | 33 (38) |
| Total | 7 (17) | 9 (45) | 41 (64) | 4 (20) | 10 (50) | 3 (27) | 74 (42) |
| Endurance | |||||||
| Women | 2 (12) | 4 (67) | 19 (68) | 8 (33) | 2 (67) | 4 (57) | 39 (46) |
| Men | 1 (20) | 3 (75) | 21 (70) | 5 (19) | 6 (55) | 2 (29) | 38 (45) |
| Total | 3 (14) | 7 (70) | 40 (69) | 13 (25) | 8 (57) | 6 (43) | 77 (46) |
| All events | |||||||
| Women | 9 (22) | 10 (71) | 41 (66) | 8 (24) | 6 (67) | 6 (46) | 80 (47) |
| Men | 1 (5) | 6 (38) | 40 (67) | 9 (24) | 12 (48) | 3 (25) | 71 (41) |
| Total | 10 (16) | 16 (53) | 81 (66) | 17 (24) | 18 (53) | 9 (36) | 151 (44) |
| Stress ECG | |||||||
| Power/strength | |||||||
| Women | 1 (4) | 4 (50) | 12 (35) | 0 (0) | 1 (17) | 0 (0) | 18 (21) |
| Men | 0 (0) | 2 (17) | 16 (53) | 2 (18) | 1 (7) | 1 (20) | 22 (25) |
| Total | 1 (3) | 6 (30) | 28 (44) | 2 (10) | 2 (10) | 1 (9) | 40 (23) |
| Endurance | |||||||
| Women | 4 (25) | 4 (67) | 15 (52) | 1 (4) | 0 (0) | 0 (0) | 24 (28) |
| Men | 1 (20) | 2 (50) | 14 (47) | 2 (7) | 2 (18) | 0 (0) | 21 (25) |
| Total | 5 (24) | 6 (60) | 29 (49) | 3 (6) | 2 (14) | 0 (0) | 45 (27) |
| All events | |||||||
| Women | 5 (13) | 8 (57) | 27 (43) | 1 (3) | 1 (11) | 0 (0) | 42 (24) |
| Men | 1 (5) | 4 (25) | 30 (50) | 4 (11) | 3 (12) | 1 (8) | 43 (25) |
| Total | 6 (10) | 12 (40) | 57 (46) | 5 (7) | 4 (12) | 1 (4) | 85 (25) |
| 12-lead rest ECG | |||||||
| Power/strength | |||||||
| Women | 5 (20) | 4 (50) | 27 (79) | 1 (10) | 5 (83) | 4 (67) | 46 (52) |
| Men | 4 (25) | 2 (18) | 22 (73) | 3 (27) | 10 (71) | 2 (40) | 43 (49) |
| Total | 9 (22) | 6 (32) | 49 (77) | 4 (19) | 15 (75) | 6 (55) | 89 (51) |
| Endurance | |||||||
| Women | 7 (44) | 4 (67) | 21 (72) | 3 (13) | 1 (33) | 5 (71) | 41 (49) |
| Men | 1 (20) | 3 (75) | 22 (73) | 8 (29) | 8 (73) | 4 (57) | 46 (54) |
| Total | 8 (38) | 7 (70) | 43 (73) | 11 (22) | 9 (64) | 9 (64) | 87 (51) |
| All events | |||||||
| Women | 12 (29) | 8 (57) | 48 (76) | 4 (12) | 6 (67) | 9 (69) | 87 (50) |
| Men | 5 (24) | 5 (33) | 44 (73) | 11 (28) | 18 (72) | 6 (50) | 89 (52) |
| Total | 17 (27) | 13 (45) | 92 (75) | 15 (21) | 24 (71) | 15 (60) | 176 (51) |
| Echocardiography | |||||||
| Power/strength | |||||||
| Women | 3 (12) | 2 (25) | 16 (47) | 0 (0) | 0 (0) | 0 (0) | 21 (24) |
| Men | 3 (20) | 0 (0) | 10 (33) | 0 (0) | 4 (29) | 2 (40) | 19 (22) |
| Total | 6 (15) | 2 (10) | 26 (41) | 0 (0) | 4 (20) | 2 (18) | 40 (23) |
| Endurance | |||||||
| Women | 2 (12) | 2 (33) | 14 (48) | 1 (4) | 2 (67) | 3 (43) | 24 (29) |
| Men | 1 (20) | 1 (25) | 13 (43) | 2 (7) | 4 (36) | 2 (29) | 23 (27) |
| Total | 3 (14) | 3 (30) | 27 (46) | 3 (6) | 6 (43) | 5 (36) | 47 (28) |
| All events | |||||||
| Women | 5 (12) | 4 (29) | 30 (48) | 1 (3) | 2 (22) | 3 (23) | 45 (26) |
| Men | 4 (20) | 1 (6) | 23 (38) | 2 (5) | 8 (32) | 4 (33) | 42 (25) |
| Total | 9 (15) | 5 (17) | 53 (43) | 3 (4) | 10 (29) | 7 (28) | 87 (25) |
| At least one PPCE | |||||||
| Power/strength | |||||||
| Women | 7 (29) | 7 (88) | 29 (85) | 1 (11) | 5 (83) | 4 (67) | 53 (61) |
| Men | 5 (33) | 3 (27) | 23 (77) | 4 (36) | 11 (79) | 3 (60) | 49 (57) |
| Total | 12 (31) | 10 (53) | 52 (81) | 5 (25) | 16 (80) | 7 (64) | 102 (59) |
| Endurance | |||||||
| Women | 7 (44) | 5 (83) | 22 (76) | 8 (33) | 2 (67) | 5 (71) | 49 (58) |
| Men | 1 (20) | 3 (75) | 23 (77) | 8 (30) | 10 (91) | 4 (57) | 49 (58) |
| Total | 8 (38) | 8 (80) | 45 (76) | 16 (31) | 12 (86) | 9 (64) | 98 (58) |
| All events | |||||||
| Women | 14 (35) | 12 (86) | 51 (81) | 9 (27) | 7 (78) | 9 (69) | 102 (59) |
| Men | 6 (30) | 6 (40) | 46 (77) | 12 (32) | 21 (84) | 7 (58) | 98 (58) |
| Total | 20 (33) | 18 (62) | 97 (79) | 21 (30) | 28 (82) | 16 (64) | 200 (58) |
| NACAC | S. America | Europe | Africa | Asia | Oceania | All | |
|---|---|---|---|---|---|---|---|
| CHE | |||||||
| Power/strength | |||||||
| Women | 7 (28) | 6 (75) | 22 (65) | 0 (0) | 4 (67) | 2 (33) | 41 (47) |
| Men | 0 (0) | 3 (25) | 19 (63) | 4 (36) | 6 (43) | 1 (20) | 33 (38) |
| Total | 7 (17) | 9 (45) | 41 (64) | 4 (20) | 10 (50) | 3 (27) | 74 (42) |
| Endurance | |||||||
| Women | 2 (12) | 4 (67) | 19 (68) | 8 (33) | 2 (67) | 4 (57) | 39 (46) |
| Men | 1 (20) | 3 (75) | 21 (70) | 5 (19) | 6 (55) | 2 (29) | 38 (45) |
| Total | 3 (14) | 7 (70) | 40 (69) | 13 (25) | 8 (57) | 6 (43) | 77 (46) |
| All events | |||||||
| Women | 9 (22) | 10 (71) | 41 (66) | 8 (24) | 6 (67) | 6 (46) | 80 (47) |
| Men | 1 (5) | 6 (38) | 40 (67) | 9 (24) | 12 (48) | 3 (25) | 71 (41) |
| Total | 10 (16) | 16 (53) | 81 (66) | 17 (24) | 18 (53) | 9 (36) | 151 (44) |
| Stress ECG | |||||||
| Power/strength | |||||||
| Women | 1 (4) | 4 (50) | 12 (35) | 0 (0) | 1 (17) | 0 (0) | 18 (21) |
| Men | 0 (0) | 2 (17) | 16 (53) | 2 (18) | 1 (7) | 1 (20) | 22 (25) |
| Total | 1 (3) | 6 (30) | 28 (44) | 2 (10) | 2 (10) | 1 (9) | 40 (23) |
| Endurance | |||||||
| Women | 4 (25) | 4 (67) | 15 (52) | 1 (4) | 0 (0) | 0 (0) | 24 (28) |
| Men | 1 (20) | 2 (50) | 14 (47) | 2 (7) | 2 (18) | 0 (0) | 21 (25) |
| Total | 5 (24) | 6 (60) | 29 (49) | 3 (6) | 2 (14) | 0 (0) | 45 (27) |
| All events | |||||||
| Women | 5 (13) | 8 (57) | 27 (43) | 1 (3) | 1 (11) | 0 (0) | 42 (24) |
| Men | 1 (5) | 4 (25) | 30 (50) | 4 (11) | 3 (12) | 1 (8) | 43 (25) |
| Total | 6 (10) | 12 (40) | 57 (46) | 5 (7) | 4 (12) | 1 (4) | 85 (25) |
| 12-lead rest ECG | |||||||
| Power/strength | |||||||
| Women | 5 (20) | 4 (50) | 27 (79) | 1 (10) | 5 (83) | 4 (67) | 46 (52) |
| Men | 4 (25) | 2 (18) | 22 (73) | 3 (27) | 10 (71) | 2 (40) | 43 (49) |
| Total | 9 (22) | 6 (32) | 49 (77) | 4 (19) | 15 (75) | 6 (55) | 89 (51) |
| Endurance | |||||||
| Women | 7 (44) | 4 (67) | 21 (72) | 3 (13) | 1 (33) | 5 (71) | 41 (49) |
| Men | 1 (20) | 3 (75) | 22 (73) | 8 (29) | 8 (73) | 4 (57) | 46 (54) |
| Total | 8 (38) | 7 (70) | 43 (73) | 11 (22) | 9 (64) | 9 (64) | 87 (51) |
| All events | |||||||
| Women | 12 (29) | 8 (57) | 48 (76) | 4 (12) | 6 (67) | 9 (69) | 87 (50) |
| Men | 5 (24) | 5 (33) | 44 (73) | 11 (28) | 18 (72) | 6 (50) | 89 (52) |
| Total | 17 (27) | 13 (45) | 92 (75) | 15 (21) | 24 (71) | 15 (60) | 176 (51) |
| Echocardiography | |||||||
| Power/strength | |||||||
| Women | 3 (12) | 2 (25) | 16 (47) | 0 (0) | 0 (0) | 0 (0) | 21 (24) |
| Men | 3 (20) | 0 (0) | 10 (33) | 0 (0) | 4 (29) | 2 (40) | 19 (22) |
| Total | 6 (15) | 2 (10) | 26 (41) | 0 (0) | 4 (20) | 2 (18) | 40 (23) |
| Endurance | |||||||
| Women | 2 (12) | 2 (33) | 14 (48) | 1 (4) | 2 (67) | 3 (43) | 24 (29) |
| Men | 1 (20) | 1 (25) | 13 (43) | 2 (7) | 4 (36) | 2 (29) | 23 (27) |
| Total | 3 (14) | 3 (30) | 27 (46) | 3 (6) | 6 (43) | 5 (36) | 47 (28) |
| All events | |||||||
| Women | 5 (12) | 4 (29) | 30 (48) | 1 (3) | 2 (22) | 3 (23) | 45 (26) |
| Men | 4 (20) | 1 (6) | 23 (38) | 2 (5) | 8 (32) | 4 (33) | 42 (25) |
| Total | 9 (15) | 5 (17) | 53 (43) | 3 (4) | 10 (29) | 7 (28) | 87 (25) |
| At least one PPCE | |||||||
| Power/strength | |||||||
| Women | 7 (29) | 7 (88) | 29 (85) | 1 (11) | 5 (83) | 4 (67) | 53 (61) |
| Men | 5 (33) | 3 (27) | 23 (77) | 4 (36) | 11 (79) | 3 (60) | 49 (57) |
| Total | 12 (31) | 10 (53) | 52 (81) | 5 (25) | 16 (80) | 7 (64) | 102 (59) |
| Endurance | |||||||
| Women | 7 (44) | 5 (83) | 22 (76) | 8 (33) | 2 (67) | 5 (71) | 49 (58) |
| Men | 1 (20) | 3 (75) | 23 (77) | 8 (30) | 10 (91) | 4 (57) | 49 (58) |
| Total | 8 (38) | 8 (80) | 45 (76) | 16 (31) | 12 (86) | 9 (64) | 98 (58) |
| All events | |||||||
| Women | 14 (35) | 12 (86) | 51 (81) | 9 (27) | 7 (78) | 9 (69) | 102 (59) |
| Men | 6 (30) | 6 (40) | 46 (77) | 12 (32) | 21 (84) | 7 (58) | 98 (58) |
| Total | 20 (33) | 18 (62) | 97 (79) | 21 (30) | 28 (82) | 16 (64) | 200 (58) |
NACAC: North American, Central American and Caribbean Athletics Association.
Examinations were clinical heart examination (CHE), 12-lead rest electrocardiogram (12-lead rest ECG), stress electrocardiogram (stress ECG), echocardiography examination and at least one pre-participation cardiac evaluation (PPCE).
Number of athletes (percentage of respondents) reporting examinations displayed by continent, event type (power/strength, endurance) and gender (women, men).
| NACAC | S. America | Europe | Africa | Asia | Oceania | All | |
|---|---|---|---|---|---|---|---|
| CHE | |||||||
| Power/strength | |||||||
| Women | 7 (28) | 6 (75) | 22 (65) | 0 (0) | 4 (67) | 2 (33) | 41 (47) |
| Men | 0 (0) | 3 (25) | 19 (63) | 4 (36) | 6 (43) | 1 (20) | 33 (38) |
| Total | 7 (17) | 9 (45) | 41 (64) | 4 (20) | 10 (50) | 3 (27) | 74 (42) |
| Endurance | |||||||
| Women | 2 (12) | 4 (67) | 19 (68) | 8 (33) | 2 (67) | 4 (57) | 39 (46) |
| Men | 1 (20) | 3 (75) | 21 (70) | 5 (19) | 6 (55) | 2 (29) | 38 (45) |
| Total | 3 (14) | 7 (70) | 40 (69) | 13 (25) | 8 (57) | 6 (43) | 77 (46) |
| All events | |||||||
| Women | 9 (22) | 10 (71) | 41 (66) | 8 (24) | 6 (67) | 6 (46) | 80 (47) |
| Men | 1 (5) | 6 (38) | 40 (67) | 9 (24) | 12 (48) | 3 (25) | 71 (41) |
| Total | 10 (16) | 16 (53) | 81 (66) | 17 (24) | 18 (53) | 9 (36) | 151 (44) |
| Stress ECG | |||||||
| Power/strength | |||||||
| Women | 1 (4) | 4 (50) | 12 (35) | 0 (0) | 1 (17) | 0 (0) | 18 (21) |
| Men | 0 (0) | 2 (17) | 16 (53) | 2 (18) | 1 (7) | 1 (20) | 22 (25) |
| Total | 1 (3) | 6 (30) | 28 (44) | 2 (10) | 2 (10) | 1 (9) | 40 (23) |
| Endurance | |||||||
| Women | 4 (25) | 4 (67) | 15 (52) | 1 (4) | 0 (0) | 0 (0) | 24 (28) |
| Men | 1 (20) | 2 (50) | 14 (47) | 2 (7) | 2 (18) | 0 (0) | 21 (25) |
| Total | 5 (24) | 6 (60) | 29 (49) | 3 (6) | 2 (14) | 0 (0) | 45 (27) |
| All events | |||||||
| Women | 5 (13) | 8 (57) | 27 (43) | 1 (3) | 1 (11) | 0 (0) | 42 (24) |
| Men | 1 (5) | 4 (25) | 30 (50) | 4 (11) | 3 (12) | 1 (8) | 43 (25) |
| Total | 6 (10) | 12 (40) | 57 (46) | 5 (7) | 4 (12) | 1 (4) | 85 (25) |
| 12-lead rest ECG | |||||||
| Power/strength | |||||||
| Women | 5 (20) | 4 (50) | 27 (79) | 1 (10) | 5 (83) | 4 (67) | 46 (52) |
| Men | 4 (25) | 2 (18) | 22 (73) | 3 (27) | 10 (71) | 2 (40) | 43 (49) |
| Total | 9 (22) | 6 (32) | 49 (77) | 4 (19) | 15 (75) | 6 (55) | 89 (51) |
| Endurance | |||||||
| Women | 7 (44) | 4 (67) | 21 (72) | 3 (13) | 1 (33) | 5 (71) | 41 (49) |
| Men | 1 (20) | 3 (75) | 22 (73) | 8 (29) | 8 (73) | 4 (57) | 46 (54) |
| Total | 8 (38) | 7 (70) | 43 (73) | 11 (22) | 9 (64) | 9 (64) | 87 (51) |
| All events | |||||||
| Women | 12 (29) | 8 (57) | 48 (76) | 4 (12) | 6 (67) | 9 (69) | 87 (50) |
| Men | 5 (24) | 5 (33) | 44 (73) | 11 (28) | 18 (72) | 6 (50) | 89 (52) |
| Total | 17 (27) | 13 (45) | 92 (75) | 15 (21) | 24 (71) | 15 (60) | 176 (51) |
| Echocardiography | |||||||
| Power/strength | |||||||
| Women | 3 (12) | 2 (25) | 16 (47) | 0 (0) | 0 (0) | 0 (0) | 21 (24) |
| Men | 3 (20) | 0 (0) | 10 (33) | 0 (0) | 4 (29) | 2 (40) | 19 (22) |
| Total | 6 (15) | 2 (10) | 26 (41) | 0 (0) | 4 (20) | 2 (18) | 40 (23) |
| Endurance | |||||||
| Women | 2 (12) | 2 (33) | 14 (48) | 1 (4) | 2 (67) | 3 (43) | 24 (29) |
| Men | 1 (20) | 1 (25) | 13 (43) | 2 (7) | 4 (36) | 2 (29) | 23 (27) |
| Total | 3 (14) | 3 (30) | 27 (46) | 3 (6) | 6 (43) | 5 (36) | 47 (28) |
| All events | |||||||
| Women | 5 (12) | 4 (29) | 30 (48) | 1 (3) | 2 (22) | 3 (23) | 45 (26) |
| Men | 4 (20) | 1 (6) | 23 (38) | 2 (5) | 8 (32) | 4 (33) | 42 (25) |
| Total | 9 (15) | 5 (17) | 53 (43) | 3 (4) | 10 (29) | 7 (28) | 87 (25) |
| At least one PPCE | |||||||
| Power/strength | |||||||
| Women | 7 (29) | 7 (88) | 29 (85) | 1 (11) | 5 (83) | 4 (67) | 53 (61) |
| Men | 5 (33) | 3 (27) | 23 (77) | 4 (36) | 11 (79) | 3 (60) | 49 (57) |
| Total | 12 (31) | 10 (53) | 52 (81) | 5 (25) | 16 (80) | 7 (64) | 102 (59) |
| Endurance | |||||||
| Women | 7 (44) | 5 (83) | 22 (76) | 8 (33) | 2 (67) | 5 (71) | 49 (58) |
| Men | 1 (20) | 3 (75) | 23 (77) | 8 (30) | 10 (91) | 4 (57) | 49 (58) |
| Total | 8 (38) | 8 (80) | 45 (76) | 16 (31) | 12 (86) | 9 (64) | 98 (58) |
| All events | |||||||
| Women | 14 (35) | 12 (86) | 51 (81) | 9 (27) | 7 (78) | 9 (69) | 102 (59) |
| Men | 6 (30) | 6 (40) | 46 (77) | 12 (32) | 21 (84) | 7 (58) | 98 (58) |
| Total | 20 (33) | 18 (62) | 97 (79) | 21 (30) | 28 (82) | 16 (64) | 200 (58) |
| NACAC | S. America | Europe | Africa | Asia | Oceania | All | |
|---|---|---|---|---|---|---|---|
| CHE | |||||||
| Power/strength | |||||||
| Women | 7 (28) | 6 (75) | 22 (65) | 0 (0) | 4 (67) | 2 (33) | 41 (47) |
| Men | 0 (0) | 3 (25) | 19 (63) | 4 (36) | 6 (43) | 1 (20) | 33 (38) |
| Total | 7 (17) | 9 (45) | 41 (64) | 4 (20) | 10 (50) | 3 (27) | 74 (42) |
| Endurance | |||||||
| Women | 2 (12) | 4 (67) | 19 (68) | 8 (33) | 2 (67) | 4 (57) | 39 (46) |
| Men | 1 (20) | 3 (75) | 21 (70) | 5 (19) | 6 (55) | 2 (29) | 38 (45) |
| Total | 3 (14) | 7 (70) | 40 (69) | 13 (25) | 8 (57) | 6 (43) | 77 (46) |
| All events | |||||||
| Women | 9 (22) | 10 (71) | 41 (66) | 8 (24) | 6 (67) | 6 (46) | 80 (47) |
| Men | 1 (5) | 6 (38) | 40 (67) | 9 (24) | 12 (48) | 3 (25) | 71 (41) |
| Total | 10 (16) | 16 (53) | 81 (66) | 17 (24) | 18 (53) | 9 (36) | 151 (44) |
| Stress ECG | |||||||
| Power/strength | |||||||
| Women | 1 (4) | 4 (50) | 12 (35) | 0 (0) | 1 (17) | 0 (0) | 18 (21) |
| Men | 0 (0) | 2 (17) | 16 (53) | 2 (18) | 1 (7) | 1 (20) | 22 (25) |
| Total | 1 (3) | 6 (30) | 28 (44) | 2 (10) | 2 (10) | 1 (9) | 40 (23) |
| Endurance | |||||||
| Women | 4 (25) | 4 (67) | 15 (52) | 1 (4) | 0 (0) | 0 (0) | 24 (28) |
| Men | 1 (20) | 2 (50) | 14 (47) | 2 (7) | 2 (18) | 0 (0) | 21 (25) |
| Total | 5 (24) | 6 (60) | 29 (49) | 3 (6) | 2 (14) | 0 (0) | 45 (27) |
| All events | |||||||
| Women | 5 (13) | 8 (57) | 27 (43) | 1 (3) | 1 (11) | 0 (0) | 42 (24) |
| Men | 1 (5) | 4 (25) | 30 (50) | 4 (11) | 3 (12) | 1 (8) | 43 (25) |
| Total | 6 (10) | 12 (40) | 57 (46) | 5 (7) | 4 (12) | 1 (4) | 85 (25) |
| 12-lead rest ECG | |||||||
| Power/strength | |||||||
| Women | 5 (20) | 4 (50) | 27 (79) | 1 (10) | 5 (83) | 4 (67) | 46 (52) |
| Men | 4 (25) | 2 (18) | 22 (73) | 3 (27) | 10 (71) | 2 (40) | 43 (49) |
| Total | 9 (22) | 6 (32) | 49 (77) | 4 (19) | 15 (75) | 6 (55) | 89 (51) |
| Endurance | |||||||
| Women | 7 (44) | 4 (67) | 21 (72) | 3 (13) | 1 (33) | 5 (71) | 41 (49) |
| Men | 1 (20) | 3 (75) | 22 (73) | 8 (29) | 8 (73) | 4 (57) | 46 (54) |
| Total | 8 (38) | 7 (70) | 43 (73) | 11 (22) | 9 (64) | 9 (64) | 87 (51) |
| All events | |||||||
| Women | 12 (29) | 8 (57) | 48 (76) | 4 (12) | 6 (67) | 9 (69) | 87 (50) |
| Men | 5 (24) | 5 (33) | 44 (73) | 11 (28) | 18 (72) | 6 (50) | 89 (52) |
| Total | 17 (27) | 13 (45) | 92 (75) | 15 (21) | 24 (71) | 15 (60) | 176 (51) |
| Echocardiography | |||||||
| Power/strength | |||||||
| Women | 3 (12) | 2 (25) | 16 (47) | 0 (0) | 0 (0) | 0 (0) | 21 (24) |
| Men | 3 (20) | 0 (0) | 10 (33) | 0 (0) | 4 (29) | 2 (40) | 19 (22) |
| Total | 6 (15) | 2 (10) | 26 (41) | 0 (0) | 4 (20) | 2 (18) | 40 (23) |
| Endurance | |||||||
| Women | 2 (12) | 2 (33) | 14 (48) | 1 (4) | 2 (67) | 3 (43) | 24 (29) |
| Men | 1 (20) | 1 (25) | 13 (43) | 2 (7) | 4 (36) | 2 (29) | 23 (27) |
| Total | 3 (14) | 3 (30) | 27 (46) | 3 (6) | 6 (43) | 5 (36) | 47 (28) |
| All events | |||||||
| Women | 5 (12) | 4 (29) | 30 (48) | 1 (3) | 2 (22) | 3 (23) | 45 (26) |
| Men | 4 (20) | 1 (6) | 23 (38) | 2 (5) | 8 (32) | 4 (33) | 42 (25) |
| Total | 9 (15) | 5 (17) | 53 (43) | 3 (4) | 10 (29) | 7 (28) | 87 (25) |
| At least one PPCE | |||||||
| Power/strength | |||||||
| Women | 7 (29) | 7 (88) | 29 (85) | 1 (11) | 5 (83) | 4 (67) | 53 (61) |
| Men | 5 (33) | 3 (27) | 23 (77) | 4 (36) | 11 (79) | 3 (60) | 49 (57) |
| Total | 12 (31) | 10 (53) | 52 (81) | 5 (25) | 16 (80) | 7 (64) | 102 (59) |
| Endurance | |||||||
| Women | 7 (44) | 5 (83) | 22 (76) | 8 (33) | 2 (67) | 5 (71) | 49 (58) |
| Men | 1 (20) | 3 (75) | 23 (77) | 8 (30) | 10 (91) | 4 (57) | 49 (58) |
| Total | 8 (38) | 8 (80) | 45 (76) | 16 (31) | 12 (86) | 9 (64) | 98 (58) |
| All events | |||||||
| Women | 14 (35) | 12 (86) | 51 (81) | 9 (27) | 7 (78) | 9 (69) | 102 (59) |
| Men | 6 (30) | 6 (40) | 46 (77) | 12 (32) | 21 (84) | 7 (58) | 98 (58) |
| Total | 20 (33) | 18 (62) | 97 (79) | 21 (30) | 28 (82) | 16 (64) | 200 (58) |
NACAC: North American, Central American and Caribbean Athletics Association.
Examinations were clinical heart examination (CHE), 12-lead rest electrocardiogram (12-lead rest ECG), stress electrocardiogram (stress ECG), echocardiography examination and at least one pre-participation cardiac evaluation (PPCE).
HDI and gender
The prevalence of athletes being provided at least one PPCE differed with regard to combinations of the HDI of the athlete's home country and gender (P = 0.005). Among athletes from HICs, the experience of at least one PPCE was more frequently reported by female athletes (P = 0.009, ϕ = 0.17; OR 3.41, 95% CI 1.34–8.71). The provision of at least one PPCE did not differ by gender in LMICs (P = 0.876), nor in VHICs (P = 0.060).
Federation health insurance
Having been provided at least one PPCE differed by combinations of gender, event category and FHI (P = 0.040). While there were no significant differences in examination patterns over gender and FHI for athletes in power/strength events (P = 0.392), there were differences for athletes in endurance events (P = 0.042). Female endurance athletes were less likely to have been provided at least one PPCE if not having FHI (P = 0.033, ϕ = 0.15; OR 0.28, 95% CI 0.09–0.94). There were no such differences among male endurance athletes (P = 0.561).
PPCE scores
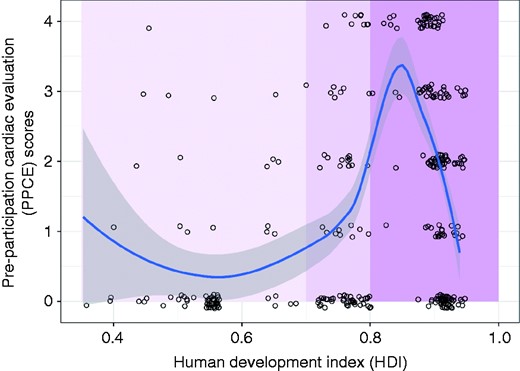
Pre-participation cardiac evaluation (PPCE) scores displayed by human development index (HDI) with Spearman's rho 0.20. The three vertically divided regions (different nuances of magenta) represent the low and middle-income countries (LMICs), high income countries (HICs) and very high income countries (VHICs). The blue line and its shaded area are estimated using locally estimated scatterplot smoothing (loess). Data points are slightly jittered for illustrative purposes.
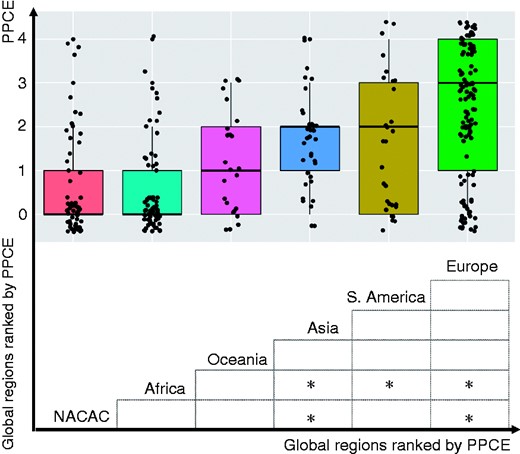
Pre-participation cardiac evaluation (PPCE) scores by global region. Upper part shows the box and whiskers plot for PPCE scores where the centre of the boxes indicate the medians, the limits of the boxes indicate the first and third quartiles, the endpoint of the vertical lines indicates the whiskers (more than 1.5 of the interquartile range outside the 1st or 3rd quartile) and dots individuals scores (jittered for illustrative purposes). The bottom part shows comparisons between PPCE scores by Kruskal–Wallis test with the Nemenyi test as a post-hoc test where * indicates significant differences. (Oceania did not differ significantly from any other region, possibly because of few participants.).
Clinical heart examination
Forty-four per cent of the participating athletes (46% of women; 41% of men) reported that they had been provided a CHE. Athletes from VHICs reported higher provision (OR 3.12, 95% CI 1.99–4.92) while athletes from LMICs (OR 0.30, 95% CI 0.16–0.54) and HICs (OR 0.59, 95% CI 0.35–1.00) reported lower provision of CHE (P < 0.001, ϕ = 0.19). Also, athletes from Europe showed higher provision of CHE (OR 4.26, 95% CI 2.66–6.81), while athletes from NACAC (OR 0.19, 95% CI 0.09–0.39) and Africa (OR 0.33, 95% CI 0.18–0.59) reported lower provision (P < 0.001, ϕ = 0.27). There were no significant differences in reports of CHE between women and men (P = 0.386).
HDI and gender
Whether or not having been provided a CHE differed by combinations of the HDI of the athlete's home country and gender (P = 0.015). Female athletes from HICs were more likely to having been provided a CHE compared with their male peers (P = 0.007, ϕ = 0.18; OR 3.78, 95% CI 1.41–10.10). There were no significant gender differences in CHE provision among athletes from LMICs (P = 0.748), or among athletes representing VHICs (P = 0.273).
Federation health insurance
Having been provided a CHE differed by combinations of gender, event category and FHI (P = 0.041). While there were no significant differences in examination patterns over gender and FHI for athletes in power/strength events (P = 0.571), there were such differences for athletes in endurance events (P = 0.023). Female endurance athletes were less likely to having been provided a CHE if not having FHI (P = 0.001, ϕ = 0.23; OR 0.16, 95% CI 0.05–0.52). There were no such differences among male endurance athletes (P = 0.779).
12-Lead rest ECG
Fifty-one per cent of the participating athletes (50% of women; 52% of men) reported that they had been provided a 12-lead rest ECG. Athletes from VHICs (OR 6.13, 95% CI 3.82–9.82) showed higher provision while athletes from LMICs (OR 0.17, 95% CI 0.09–0.31) and HICs (OR 0.40, 95% CI 0.24–0.68) showed lower provision of 12-lead rest ECG (P < 0.001, ϕ = 0.29). Also, athletes from Europe (OR 4.76, 95% CI 2.92–7.76) and from Asia (OR 2.72, 95% CI 1.27–5.83) showed higher provision of 12-lead rest ECG examinations, while athletes from NACAC (OR 0.29, 95% CI 0.16–0.53) and Africa (OR 0.18, 95% CI 0.10–0.34) reported lower provision (P < 0.001, ϕ = 0.31). There were no significant differences in reports of 12-lead rest ECG between women and men (P = 0.787).
HDI and gender
Whether or not having been provided a 12-lead rest ECG differed by combinations of the HDI of the athlete's home country and gender (P = 0.031). Female athletes from HICs were more likely to be provided a CHE than their male peers (P = 0.078) while male athletes were more likely to be provided a 12-lead rest ECG if coming from LMICs (P = 0.134) or VHICs (P = 0.131) (only difference between patterns statistically significant).
Federation health insurance
Whether or not having been provided a 12-lead rest ECG did not differ depending on having FHI or not (P = 0.696).
Stress ECG
Twenty-five per cent of the participating athletes (25% of women; 25% of men) reported that they had been provided a stress ECG. Athletes from VHICs (OR 2.33, 95% CI 1.33–4.06) reported higher provision while athletes from LMICs (OR 0.20, 95% CI 0.08–0.52) reported lower provision of stress ECG (P < 0.001, ϕ = 0.14). Also, athletes from Europe (OR 6.65, 95% CI 3.82–11.58) and South America (OR 2.21, 95% CI 1.02–4.82) showed higher provision of stress ECG examination while their peers from NACAC (OR 0.29, 95% CI 0.12–0.69), Africa (OR 0.18, 95% CI 0.06–0.52), Asia (OR 0.09, 95% CI 0.01–0.65) and Oceania (OR 0.12, 95% CI 0.02–0.87) showed lower provision (P < 0.001, ϕ = 0.30). There were no significant differences in reports of stress ECG between women and men (P = 0.951).
HDI and gender
Differences in provision of stress ECG between women and men did not differ significantly over countries with different HDI (P = 0.068).
Federation health insurance
Provision of stress ECG was differently distributed with regard to gender and FHI (P = 0.036). Women were more often provided a stress ECG when having FHI (P = 0.176) while the pattern was opposite among men (P = 0.103) (only difference between patterns statistically significant).
Trans-thoracic echocardiography
Twenty-five per cent of the participating athletes (26% of women; 25% of men) reported that they had been provided a TTE. Athletes from VHICs (OR 3.65, 95% CI 2.03–6.58) reported higher provision while their peers from LMICs (OR 0.15, 95% CI 0.05–0.42) reported lower provision of TTE (P < 0.001, ϕ = 0.18). Also, athletes from Europe (OR 4.18, 95% CI 2.48–7.02) showed higher provision of TTE, while athletes from NACAC (OR 0.45, 95% CI 0.21–0.95) and Africa (OR 0.12, 95% CI 0.04–0.40) showed lower provision (P < 0.001, ϕ = 0.23). There were no significant differences in reports of TTE between women and men (P = 0.712).
Federation health insurance
At the athlete level, TTE differed by combinations of gender, event category and FHI (P = 0.005). There were significant differences in examination patterns over event category and FHI for men (P = 0.001) but not for women (P = 0.474). For male athletes participating in power/strength events, FHI was associated with more TTE (P = 0.011; OR 3.86, 95% CI 1.32–11.25), while for male athletes participating in endurance events FHI was associated with less TTE (P = 0.040; OR 0.26, 95% CI 0.07–1.00).
Discussion
IAAF, as the athletics governing body, counts 214 national federations, and athletics is thereby the most globally representative sport.10 Having so many different events within athletics and being so inclusive, allows talented athletes to compete against each other regardless of their country national income or individual sociodemographic background. This makes the detection of clinically relevant conditions among athletes competing at international championships a real challenge. Similarly to a study conducted at the Rio Olympics,11 we found a large difference in PPCE prevalence between athletes from LMICs (28%) and VHICs (74%). We also found that the TTE prevalence among African athletes was low (4%). These are concerning findings due to the fact that non-training-related ECG abnormalities have been reported to be three to four times more common in athletes of African descent than among their peers with Arab or Caucasian origin.12 Data from adult athletes of African descent have shown an almost fivefold increase in left ventricular (LV) hypertrophy on echocardiography compared with Caucasian athletes.13 The specificity of these variations has been further highlighted in several studies involving only athletes of African descent.14,–16 These studies have reported that the prevalence of an abnormal ECG, in particular T wave inversion, differed by geographical origin, with athletes of West and Central African descent having higher rates of abnormal findings. Furthermore, athletes from West, Central Africa and the Caribbean also had a greater LV wall thickness and LV mass compared with athletes from East Africa and West Asia. These observations should be interpreted in parallel with the fact that the likelihood of different CVDs, congenital and acquired, differs considerably between athletes depending on their geographical residence and genetic background. For instance, while RHD has almost been eradicated in VHICs, an echocardiographic study involving school children aged 5–16 years in Uganda found a 1.5% prevalence,17 and an Eritrean study involving high school populations reported that 4% had definitive RHD and 3.3% suspected RHD.18 Such complexity has led to the fact that no best practice cardiac evaluation protocol, that allows us to differentiate between physiological adaptations to training, genetic variations and clinically relevant CVD, among athletes of various descent, has yet been established. Recently, needs have been expressed for more specific information about athlete-level PPCE within global regions,11 while substantial local variations in cardiac disease prevalence have also been reported.19 The applicability of a unique solution and universally adoptable approach remains challenging in the athletics worldwide scenario. A tailored approach is most likely the appropriate solution, as it has been demonstrated in other specific contexts.20,21 Such a tailored approach should be based on geographical diseases prevalence. The findings of this study imply that the provision of PPCE in LMICs, and athletes of African descent, in particular, needs urgent attention.
This study showed that the athletes' PPCE scores increased with the HDI of their home country, but also that there was a considerable proportion of athletes with low PPCE scores at the very highest developmental level. This could be explained by a lack of available health insurance covering cardiac preventive actions for athletes from VHICs or that country-specific rules and/or regulations applied. Regarding variations in PPCE prevalence, our study showed some unexpected results. Having FHI showed little association with PPCE provision in general. This may be explained by the fact that medical insurance did not cover preventive services and that FHI plans need to be expanded accordingly.22 However, having health insurance still appeared helpful as stress ECG and CHE (endurance events) were more often performed among female athletes, when compared with their peers without insurance.23 Our report of athletes with low formal education displaying higher PPCE scores is an interesting finding. This information strictly reflects the European sports system as well as the actual dual career limitations. It is more common in Europe, than in other regions, to reach the elite level in the sports without in parallel having progressed in the formal educational system. The same phenomenon was observed comparing the athletes' formal education with their country HDI, i.e. there was a larger proportion with high education among athletes originating from LMICs and a larger proportion with low education among athletes from nations in the VHIC category. A plausible reason for this discrepancy can be found in the sports scholarships system that is highly predominant in certain regions of the world and that is also able to attract athletes from LMICs. The results of this study suggest that besides global differences in PPCE prevalence, uncoordinated mechanisms, both primary compensatory and secondary accidental, influence athlete-level inequity in the provision of PPCE. This should be considered when designing future preventive campaigns.
Study limitations
When interpreting the results, some limiting factors must be considered. This is the first study to assess PPCE patterns among athletes competing at athletics WCH and, also the first report of PPCE data on an individual sport, at elite level. Our study shows a lower response rate among participants at the London IAAF WCH (39% of participating athletes took part to the survey). The reduction was associated with social distancing measures enforced by public health authorities to control a norovirus outbreak. As difficulties to reach out to the athletes were unrelated to the study objectives, it is unlikely that the virus outbreak influenced the athletes' response and the study conclusions. Finally, the prevalence of CVDs was not assessed in this study, which should be an area of future research.
In our elite athletic study population, slightly more than 50% of the athletes had been provided some type of PPCE, while TTE and stress ECG had been provided to only one out of four participants. These low rates were observed despite the existence of specific recommendations for PPCE issued by the IAAF in 2013.24 The practical implementation of these recommendations is still far from providing geographically equal access to prevention for athletes competing at the highest level in athletics. Indeed, athletes from LMICs reported lower provision rates for all types of PPCE compared with athletes from VHICs, and athletes from Africa and NACAC reported lower provision rates compared with athletes from Europe. This is worrying because even though rare, SCD represents the leading medical cause of death in young athletes, with male athletes of African or Caribbean descent at particular risk.25 It seems likely that one of the greatest challenges for the implementation of preventive recommendations is the lack of resources in LMICs and HICs, while at the same time in some VHICs country-specific regulations may limit the adoption of these preventive measures. Being aware of the ongoing debate between scientists supporting PPCE and those in favour of an informed and educational approach, we believe this information, coming from a real international scenario, is useful.26,27 These challenges represent a call to the experts in the fields of sports cardiology and sports medicine to find solutions that could be applicable also in countries with limited financial, infrastructural or educational resources. International sports federations should play a role in protecting athletes' health and promoting their wellbeing.28 Ideally this should be achieved through a comprehensive approach that relies on science-based regulations, widespread education and equal access to resources. In conclusion, our study shows that provision of PPCE in LMICs, and the African countries in particular, needs urgent attention and that increases in evaluation prevalence should be accompanied by the development of cost-effective methods that are applicable in all global regions.
Supplemental Material
CPR884385 Supplemental Material - Supplemental material for Efficacy of pre-participation cardiac evaluation recommendations among athletes participating in World Athletics Championships
Supplemental material, CPR884385 Supplemental Material for Efficacy of pre-participation cardiac evaluation recommendations among athletes participating in World Athletics Championships by Örjan Dahlström, Paolo Emilio Adami, Kristina Fagher, Jenny Jacobsson, Victor Bargoria, Håkan Gauffin, Per-Olof Hansson, Christer Andersson, Stéphane Bermon and Toomas Timpka in European Journal of Preventive Cardiology
Author contribution
OD, PEA, KF, JJ, VB, HG, POH, CA, SB and TT contributed to the conception or design of the work. OD, PEA, KF, JJ, VB, HG, POH, CA, SB and TT contributed to the acquisition, analysis, or interpretation of data for the work. OD, PEA and TT drafted the manuscript. OD, PEA, KF, JJ, VB, HG, POH, CA, SB and TT critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work ensuring integrity and accuracy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.

{kind=link}
{kind=link}
Comments