Article Text

Abstract
Purpose This study evaluated the association between ischaemic stroke (IS) and heart failure (HF) in the absence of atrial fibrillation (AF) or atrial flutter (AFL) using a population-based nation-wide cohort database.
Method Newly diagnosed patients with HF without previous stroke and acute myocardial infarction (AMI) were enrolled. Based on the propensity scores matching age, sex and all comorbidities, our studies comprised 12 179 patients with HF and 12 179 patients without HF. Cox proportion hazard regression models and competing-risk regression models were used to evaluate the risk of IS among patients with HF without AF or AFL.
Results In the multivariable analysis, older age (adjusted HR (95% CI)=1.05 (1.04 to 1.05)), male sex (adjusted HR (95% CI)=1.36 (1.24 to 1.50)), diabetes (adjusted HR (95% CI)=2.22 (1.97 to 2.49)) and hypertension (adjusted HR (95% CI)=1.60 (1.41 to 1.82)) were markedly associated with IS in patients with HF. The HF group had a markedly higher risk of IS than did the non-HF group (subdistribution HR (SHR)=1.51, 95% CI: 1.37 to 1.66) and AMI (SHR=3.40, 95% CI: 2.71 to 4.28). Additionally, according to the Kaplan-Meier analysis, patients with HF were at a significantly higher risk of cumulative incidence of IS and AMI than did patients with non-HF (p value of log-rank test <0.001).
Conclusion This study indicated that HF is a strong independent risk factor for IS, even in the absence of AF or AFL. Clinical physicians should investigate IS through routine screening and careful monitoring of patients with HF.
- Ischaemic stroke
- heart failure
- hemorrhagic stroke
- Taiwan National Health Insurance Research Database
Statistics from Altmetric.com
Introduction
Heart failure (HF) is a widespread medical condition and a major cause of hospitalisation, death and comorbidity worldwide.1 HF is a complex clinical syndrome characterised by dysfunction of diastole or systole of the ventricle through either structural or functional abnormalities. Common predisposing factors of HF include hypertension, valvular heart disease, diabetes, atrial fibrillation (AF), coronary artery disease (CAD) and alcohol consumption.2–4 Currently, the latest evidence-based medical treatment for HF has markedly improved the survival rate, major adverse cardiovascular events (MACE) and re-hospitalisation. However, the risk of stroke among patients with HF has considerably increased than in the past.1 Moreover, the risk of silent stroke, which is defined as ischaemic brain lesions without obvious clinical symptoms, is two to three times higher in patients with HF than in those without HF.5–7 Such evidence highlights the increasing disease burden of stroke in patients with HF even under promising therapeutic medications for HF.
Patients with ischaemic stroke (IS) have a long hospitalisation duration, poor quality of life, disability, long-term complications and a high probability of mortality. Additionally, IS has been the leading cause of hospitalisation, mortality, disability and comorbidity worldwide. Risk factors for IS are similar to those of HF, including diabetes mellitus, hypertension, obesity, CAD and AF.1 5 8 Patients with simultaneous HF and IS have more severe neurological deficits than those with stroke only.1 5 6 HF is a definite risk factor in AF to predict the probability of IS within the CHA2DS2-VACs score.5 Nearly 10%–25% of patients with IS have HF. AF occurs in 57% of patients with HF, which contributes the most to the incidence of stroke.7 9 10 The coexistence of HF and AF brings the synergistic risk of IS development, which is not as prevalent in the presence of either HF or AF. These results summarise the vital roles of AF in patients with IS and HF.
Few studies have evaluated the association of IS with HF in patients without AF or atrial flutter (AFL). Most of these studies have a small sample size and did not evaluate confounding factors including incident AF/AFL and anticoagulants.7 10 11 Therefore, we conducted a national population-based cohort study to evaluate the risk of IS in patients with HF without AF or AFL and identified potential risk factors linking these two diseases, which is beneficial for further stroke prevention in patients with HF but without AF or AFL.
Methods
Data source
The extent of insured Taiwanese population under the Taiwan National Health Insurance programme (Taiwan NHI) was over 99%. The Taiwan National Health Insurance Database (NHIRD) was established and updated once a year from 1996. We retrieve data from LHID2000. The LHID2000 contains all medical claims data for a random sampling of 1 000 000 beneficiaries from the whole insurants (23.74 million people). According to the NHRID, no statistically significant differences exist regarding the distribution of sex, age or healthcare costs between cohorts in LHID2000 and all insurants. The database contains abundant health and medical treatment information of insured individuals including their diagnoses history in a coded of the International Classification of Disease, Ninth Revision, Clinical Modification (ICD-9-CM).
Patient and public involvement
In the HF cohort, patients newly diagnosed with HF (ICD-9-CM code 428) between January 2000 and December 2012 were enrolled. The date of the first diagnosis was defined as the index date. We excluded patients with AF (ICD-9-CM code 427.31) and AFL (ICD-9-CM code 427.32) who were diagnosed before the index date or during the follow-up period. Additionally, we excluded patients with a previous history of stroke (ICD-9-CM codes 430–438) and acute myocardial infarction (AMI; ICD-9-CM code 410) at baseline.
We used propensity score for selecting the non-HF cohort by matching age, sex, monthly income, urbanisation level and certain comorbidities.12 Patients with HF were matched (1:1 ratio) with those without HF by their propensity score through nearest neighbour matching, initially to the eighth digit and then as required to the first digit. Therefore, matches were first made within a calliper width of 0.0000001, and then the calliper width was increased for unmatched cases to 0.1. We reconsidered the matching criteria and performed a rematch (greedy algorithm). For each patient with HF, the corresponding comparisons were selected based on the nearest propensity score. The C-statistic of the logistic regression model was 0.75. The presence of the following pre-existing comorbidities for each patient were identified at baseline: diabetes (ICD-9-CM code 250), hypertension (ICD-9-CM codes 401–405), hyperlipidaemia (ICD-9-CM code 272), chronic kidney disease (CKD) (ICD-9-CM codes 250.4, 274.1, 283.11, 403.1, 404.2, 404.3, 404.1, 442.1, 447.3, 580–583, 585, 587, 792.5, 642.1 and 646.2), chronic obstructive pulmonary disease (ICD-9-CM codes 490–496), peripheral vascular disease (ICD-9-CM codes 440.20–440.24, 440.9, 443.81, 443.9 and 444.22), alcohol-related illness (ICD-9-CM codes 291, 303, 305, 357.5, 425.5, 535.3, 571 and E860.0), mild liver diseases (ICD-9-CM codes 571.2, 571.3, 571.5 and 573.8), obesity (ICD-9-CM code 278.0), autoimmune disease (ICD-9-CM codes 135, 279.49, 283, 443, 571.42, 696, 710, 714 and 715), depression (ICD-9-CM codes 296.2, 296.3, 300.4 and 311), anxiety (ICD-9-CM code 300), all cancer types (ICD-9-CM codes 140–208), trauma (ICD-9-CM codes 365.65, 366.2, 376.47, 376.52, 380.51, 381.1, 518.5, 598.1, 664.8, 664.9, 665, 665.8, 665.9, 716.1, 721.7, 728.12, 860, 878, 885, 886, 887, 895, 896, 897, 958, 958.4, 958.5, 958.7 and 958.8) and CAD (ICD-9-CM codes 411–414). The same exclusion criteria were used for non-HF cohort (figure 1).
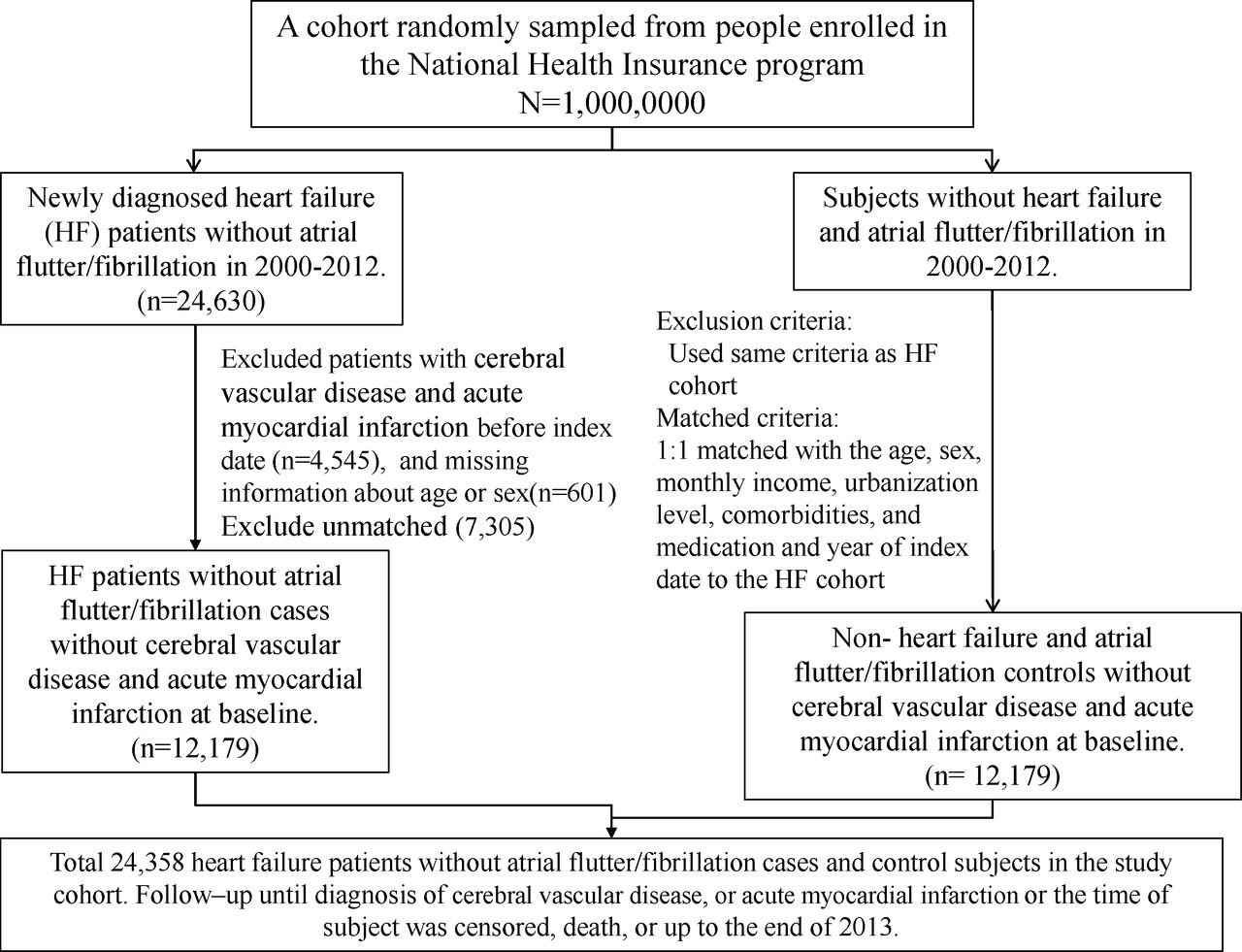
Flow chart of the study design.
The endpoint for follow-up was the date of withdrawal from the programme in patients who developed one of the outcome diseases, namely IS (ICD-9-CM codes 433–435), haemorrhagic stroke (HS) (ICD-9-CM codes 430–432) and AMI. The follow-up endpoint in patients without event was the last follow-up date (31 December 2013).
Statistical analysis
Distributions of age, sex, monthly income, urbanisation level and comorbidities in HF and non-HF cohorts are shown in numbers and percentage. The difference between the two cohorts was tested by calculating standardised mean differences, in which a value less than 0.1 indicated a negligible difference between the two cohorts. HRs and 95% CIs were estimated using Cox proportional hazard models for evaluating the association of HF with stroke, IS, HS and AMI. To address the concern of constant proportionality, we examined the proportional hazard model assumption using a test of scaled Schoenfeld residuals. There was no significant relationship between Schoenfeld residuals for HF and follow-up time (p value=0.67) in the model of evaluating IS. Interestingly, there was significant relationship between Schoenfeld residuals for HF and follow-up time in the models of evaluating stroke, HS and AMI (p value=0.003, <0.0001, 0.0001, respectively). In the subsequent analyses, we stratified the follow-up duration to deal with the violation of proportional hazard assumption. A multivariate Cox proportional hazard model was used to estimate adjusted HRs after adjustment for age, sex, monthly income, urbanisation level and all comorbidities.
We used the Fine and Grey model which extends the standard Cox proportional hazard regression model to estimate the subdistribution HR of the stroke, IS, HS and AMI, after evaluating the competing risk of deaths. The subdistribution HR (SHR) and 95% CIs were calculated using the competing-risk regression model.13 The cumulative incidence curves of stroke and AMI were plotted using the Kaplan-Meier method, and the difference between the HF and non-HF cohorts was tested using the log-rank test. All statistical analyses were performed using SAS statistical software, V.9.4 (SAS Institute, Cary, NC, USA). The Kaplan-Meier plot was plotted using R software. Statistical significance was determined using two‐tailed tests (p < 0.05).
Results
The baseline characteristics of patients are shown in table 1. Each group consisted of 12 179 patients (HF and non-HF cohorts). Except in the subgroup of patients older than 65 years, each subgroup was consistent in age, sex, monthly income, urbanisation level and all comorbidities of participants in the two cohorts (standardised mean difference <0.1).
Baseline characteristics of patients, by the presence of HF, and after matching for propensity score
Mean follow-up times were 6.54 and 5.70 years in the HF cohort and non-HF cohort, respectively. Compared with patients with non-HF, patients with HF had a significantly higher risk of stroke, IS, HS and AMI; adjusted HRs (95% CI) were 1.59 (1.46–1.74), 1.59 (1.45–1.75), 1.55 (1.27–1.90) and 3.60 (2.86–4.53), respectively (table 2).
Incidence and HR of stroke, IS, HS and AMI in patients with atrial flutter compared with those without heart failure
The association of sex, age and comorbidities with IS, HS and AMI is shown in table 3. In multivariable models, old age (adjusted HR (95% CI)=1.05 (1.04 to 1.05)), male sex (adjusted HR (95% CI)=1.36 [1.24 to 1.50]), lower monthly income (adjusted HR (95% CI)=1.38 (1.22 to 1.57)), lower urbanisation level (adjusted HR (95% CI)=1.30 (1.14 to 1.49)), diabetes (adjusted HR (95% CI)=2.22 (1.97 to 2.49)) and hypertension (adjusted HR (95% CI)=1.60 (1.41 to 1.82)) were significantly associated with IS. Patients with cancer (adjusted HR (95% CI)=0.72 (0.55 to 0.94)) had a significantly negative association with IS. Old age (adjusted HR (95% CI)=1.02 (1.01 to 1.03)), male sex (adjusted HR (95% CI)=1.44 (1.17 to 1.77)), lower monthly income (adjusted HR (95% CI)=1.94 (1.49 to 2.54)), diabetes (adjusted HR (95% CI)=1.43 (1.07 to 1.91)), hypertension (adjusted HR (95% CI)=2.08 (1.58 to 2.72)) and alcohol-related illness (adjusted HR (95% CI)=1.89 (1.14 to 3.11)) were significantly associated with HS. Patients with hyperlipidaemia (adjusted HR (95% CI)=0.72 (0.57 to 0.90)) or anxiety (adjusted HR (95% CI)=0.73 (0.56 to 0.96)) had a significantly lower adjusted HR for HS. Old age (adjusted HR (95% CI)=1.04 (1.03 to 1.05)), male sex (adjusted HR (95% CI)=2.09 (1.70 to 2.57)), comorbid diabetes (adjusted HR (95% CI)=2.71 (2.12 to 3.47)), hypertension (adjusted HR (95% CI)=1.40 (1.09 to 1.81)), CKD (adjusted HR (95% CI)=1.34 (1.06 to 1.70)), CAD (adjusted HR (95% CI)=1.63 (1.26 to 2.11)) and warfarin (adjusted HR (95% CI)=2.41 (1.13 to 5.13)) were significantly associated with AMI.
HRs of outcome in association with gender, age and comorbidities in univariable and multivariable Cox proportional hazard regression models
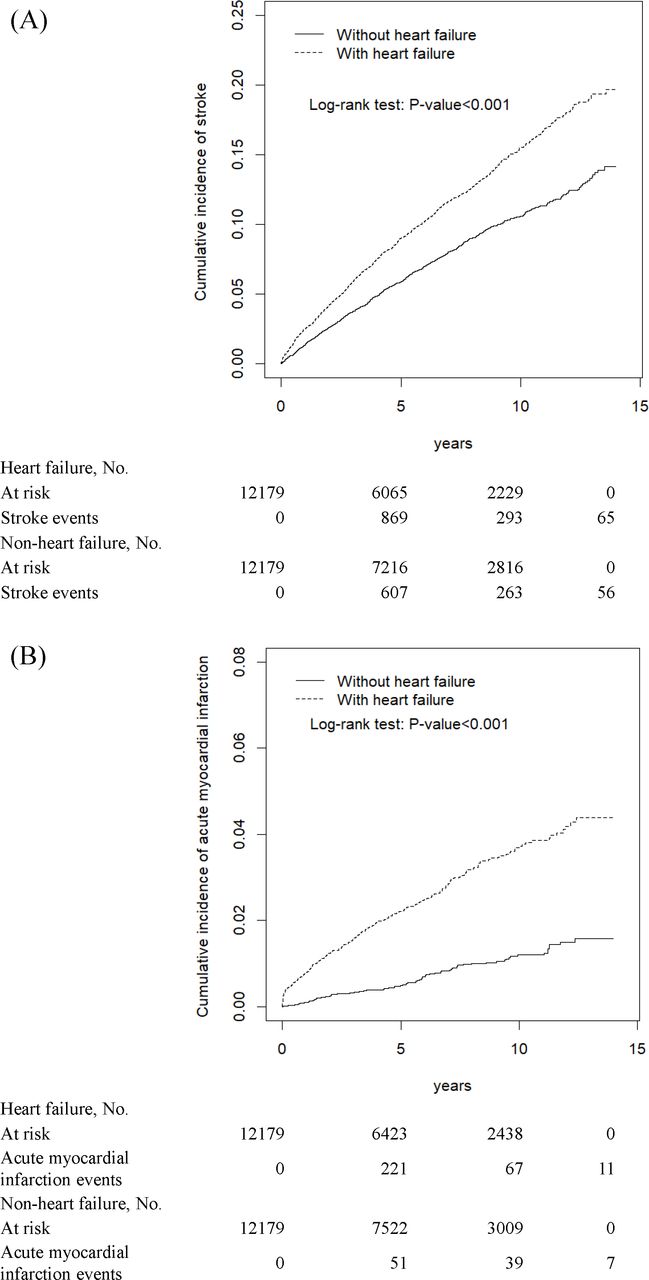
Table 4 shows the adjusted SHR after considering death as a competing outcome. The HF group was compared with the non-HF group. After adjustment for all the variables listed in table 1, there was a significantly higher risk of stroke (SHR=1.50, 95% CI: 1.38 to 1.63), IS (SHR=1.51, 95% CI: 1.37 to 1.66), HS (SHR=1.45, 95% CI: 1.19 to 1.77) and AMI (SHR=3.40, 95% CI: 2.71 to 4.28) in the HF group. The higher risk of stroke, HS and AMI occurred during the first 1 year of follow-up period in patients with HF compared with those without HF, while the trend reduced in the follow-up period of 2–4 years and >5 years (table 5). The cumulative incidences of stroke and AMI are illustrated in figure 2. Patients with HF had a significantly higher cumulative incidence of stroke and AMI than did those without HF during the follow-up periods (p value of log-rank test <0.001).
{kind=link}
{kind=link}
Cumulative incidence of ischaemic stroke (A) and acute myocardial infarction (B) in individuals with HF or without HF by propensity score matching. HF, heart failure.
Incidence and SHR of stroke, IS, HS, and AMI in propensity score-matched cohorts, using the competing-risks regression models
Incidence ratio and HR of stroke, HS and AMI in patients with/without heart failure stratified by follow-up period
Discussion
In this study, the relationship among HF without AF or AFL, stroke, IS, HS and AMI were comprehensively investigated. Our results consistently exhibited HF as a significant independent risk factor for stroke, IS, HS and AMI after adjustment for comorbidities and medication with warfarin. Risk factors for IS among patients with HF without AF or AFL were old age, male sex, low urbanisation level and diabetes. Among these, diabetes was the strongest risk factor for IS and AMI in patients with HF without AF or AFL. These results indicate that HF is an independent risk factor for IS and AMI even in the absence of AF or AFL. Our study findings remind both physicians and patients to carefully screen for IS and AMI in patients with HF without AF or AFL, especially those with diabetes.
In this study, we used the nation-wide population-based cohort from the NHIRD, which includes all Taiwanese residents. The rate of lost to follow-up was low in the longitudinal design, including both study and control cohorts. Additionally, due to the universal reimbursement policy in Taiwan, all insurance claims should be evaluated according to the standard diagnosed criteria by medical reimbursement specialists. The doctors or hospitals will be punished with huge penalties when they make wrong diagnoses or coding. Such polices contribute to the highly reliable diagnoses of IS, HF, AF/AFL based on ICD-9 codes in this study.
Several pathophysiologic mechanisms underlying stroke and HF have been proposed. In previous studies, AF and left ventricular (LV) dysfunction were the most commonly pathophysiologic mechanisms underlying thrombus formation.10 14 HF with or without LV dysfunction containing Virchow’s triad (abnormalities with circulatory stasis, hypercoagulable state and endothelial abnormality) contributes to the development of stroke.15 16 First, the hypercoagulable state among patients with HF with activation of the renin–angiotensin–aldosterone system and increasing the sympathetic nerve system results in exaggeration of platelet aggregation and hypofibrinolysis.15 17 Second, endothelial abnormality among patients with HF due to common risk factors of hypertension and diabetes is significantly associated with high von Willebrand factor levels and impairment of endothelium-derived nitric oxide (NO) leading to hypercoagulable condition.15 16 Third, circulatory stasis resulting from enlargement of the left atrium or ventricle and systolic dysfunction contribute to thrombus formation.10 18 19 Furthermore, hypoperfusion of cerebral blood flow in patients with HF with decreasing cardiac output and cerebral autoregulation dysfunction is a documented mechanism for stroke. Finally, elevation of arterial stiffness and reduction of vasodilatory reserve with reducing cerebral blood flow are proposed as pathological mechanisms for stroke.20 21 All results including abnormalities with circulatory stasis, hypercoagulable state, endothelial abnormality and hypoperfusion of cerebral blood flow elucidate a strong association between HF and stroke.
Our study demonstrated that the adjusted HR of IS and HS in patients with HF was 1.59 and 1.55, respectively, which is similar to that reported in studies involving patients from Denmark and Korea.5 22 Kang et al evaluated the risk of IS in 5746 hospitalised patients with HF, which may be contaminated with occult AF.5 Adelborg et al proposed that HF is associated with a short-term risk of IS, but the long-term risk of IS among patients with HF was lower than that in the general population, which may be due to competing mortality.22 By matching the propensity scores, our study examined 12 179 patients with HF and 12 179 patients without HF and found that patients with HF had a significantly higher cumulative incidence of IS than those without HF during the follow-up period (figure 1), which supports the strong association between HF and IS. Moreover, in contrast to containing 10% of patients with HF with AF or AFL in studies from Korean and Danish cohorts, we excluded AF or AFL in our study and minimised the confounding of AF/AFL and medications with warfarin on the association between HF and IS.5 22 Interestingly, our studies suggested male was a risk factor for IS in the HF group, which was a different outcome compared with Danish and Korean cohorts. Although the Danish cohort indicated that men and women carry equal risk of IS, Korean cohorts revealed that women had a higher risk of IS than men.5 22 Such discrepancies may be attributed to the difference in racial groups participating in these studies.
Our study proposed that diabetes carries a strong adjusted HR of IS in patients with HF, which is consistent with the observation from Melgaard et al.23 Several mechanisms explain the occurrence of IS in patients with diabetes. Diabetes impairs NO-mediated vasodilation in vascular endothelium and smooth muscle, resulting in endothelial dysfunction.23–25 Additionally, oxidised and glycated low-density lipoproteins in patients with diabetes contribute to the development of atherosclerosis. High levels of hypercoagulable and pro-inflammatory mediators, including plasminogen activator inhibitor-I, interleukin-1, interleukin-6, tumour necrosis factor-α, C-reactive proteins, activation of NFκB and Matrix Metallopeptidase 9, are commonly found in patients with diabetes and atherosclerotic cardiovascular disease.23 25 26 Furthermore, the hypercoagulable condition involved in cerebrovascular events is associated with the thrombotic state by increasing platelet activation and the level of all clotting factors.25 27 28 The combination of the hypercoagulable condition and endothelial dysfunction in patients with HF and diabetes explains the risk of IS among patients with HF and diabetes.
Our study indicated that the association of IS and HF is significant in patients who have the monthly salary of 15 000–20 000 than who have higher income. Blue-collar workers have low income and reside in areas that lack proper sanitation facilities. These people lack awareness about personal health, disease occurrence and disease prevention. The medication compliance is a significant concern among these people. Additionally, medical resources are insufficient in low urbanised areas, which contributes to the elevated risk of stroke in patients with HF.29 30
Limitations
Several limitations in our study should be pointed out. First, our NHIRD did not record life habit-related risk factors in detail, including cigarette smoking, alcohol drinking, accurate body mass index, socioeconomic condition and family history. Second, occult AF still could not be totally excluded despite the efforts to exclude all the ICD-9-CM codes of AF and AFL from the index date and follow-up period. Third, the retrospective cohort study is usually lower evidence than the randomised controlled trials because a retrospective cohort study is subject to have many unknown or uncontrolled confounding factors. Last, this study is required a large prospective study to clarify that the benefit of anticoagulants, including warfarin or novel oral anticoagulants, for stroke prevention in patients with HF without AF or AFL. Regardless of above limitations, this study provided significant evidence on the risk of IS among patients with HF without AF or AFL.
Conclusion
In this study, we concluded that HF without AF or AFL is a strong independent risk factor for IS, particularly with old age (>65 years of age), male sex, low income, low urbanisation and diabetes. This study emphasised awareness regarding IS among patients with HF, even without AF or AFL. A large prospective study is warranted to evaluate the use of anticoagulants for such patients.
Key messages
What is already known about this subject?
The risk of ischaemic stroke (IS) among patients with heart failure (HF) in the absence of atrial fibrillation (AF) or atrial flutter (AFL) had not been explored extensively.
What does this study add?
This study indicated that HF is a strong independent risk factor for IS, even in the absence of AF or AFL.
How might this impact on clinical practice?
Clinical physicians should investigate IS through routine screening and careful monitoring of patients with HF.
References
Footnotes
C-SL and C-HK contributed equally.
Contributors All authors have contributed substantially to, and are in agreement with the content of, the manuscript: Conception/Design: Y-LC, C-HK; Provision of study materials: C-HK; Collection and/or assembly of data: Y-LC, C-SL, C-LL, C-HK; Data analysis and interpretation: All authors; Manuscript preparation: All authors; Final approval of manuscript: All authors.
Funding This study is supported by the grants from Tri-Service General Hospital (TSGH-C107-007-007-S02 to C-SL), Ministry of National Defense-Medical Affairs Bureau (MAB-106-082 to C-SL) and Taiwan Ministry of Science and Technology (MOST 106-2314-B-016-038-MY3 to C-SL), Taiwan Ministry of Health and Welfare Clinical Trial Center (MOHW108-TDU-B-212-133004), China Medical University Hospital, Academia Sinica Stroke Biosignature Project (BM10701010021), MOST Clinical Trial Consortium for Stroke (MOST 108-2321-B-039-003-), Tseng-Lien Lin Foundation, Taichung, Taiwan, and Katsuzo and Kiyo Aoshima Memorial Funds, Japan.
Disclaimer The funders had no role in study design, data collection or analysis, decision to publish or preparation of the manuscript. No additional external funding was received for this study.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The Research Ethics Committee of China Medical University and Hospital in Taiwan approved the study (CMUH104-REC2-115-R4).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.