Peripartum cardiomyopathy
BMJ 2019; 364 doi: https://doi.org/10.1136/bmj.k5287 (Published 30 January 2019) Cite this as: BMJ 2019;364:k5287
- Michael C Honigberg, clinical and research fellow in cardiology1 3,
- Michael M Givertz, medical director, professor of medicine2 3
- 1Cardiology Division, Department of Medicine, Massachusetts General Hospital, Boston, MA, 02114, USA
- 2Cardiovascular Division, Department of Medicine, Brigham and Women’s Hospital, Boston, MA 02115, USA
- 3Harvard Medical School, Boston, MA, 02115, USA
- Correspondence to: M M Givertz mgivertz{at}bwh.harvard.edu
Abstract
Peripartum cardiomyopathy (PPCM) is a rare, often dilated, cardiomyopathy with systolic dysfunction that presents in late pregnancy or, more commonly, the early postpartum period. Although the condition is prevalent worldwide, women with black ancestry seem to be at greatest risk, and the condition has a particularly high incidence in Nigeria and Haiti. Other risk factors include pre-eclampsia, advanced maternal age, and multiple gestation pregnancy. Although the complete pathophysiology of peripartum cardiomyopathy remains unclear, research over the past decade suggests the importance of vasculo-hormonal pathways in women with underlying susceptibility. At least some women with the condition harbor an underlying sarcomere gene mutation. More than half of affected women recover systolic function, although some are left with a chronic cardiomyopathy, and a minority requires mechanical support or cardiac transplantation (or both). Other potential complications include thromboembolism and arrhythmia. Currently, management entails standard treatments for heart failure with reduced ejection fraction, with attention to minimizing potential adverse effects on the fetus in women who are still pregnant. Bromocriptine is one potential disease specific treatment under investigation. In this review, we summarize the current literature on peripartum cardiomyopathy, as well as gaps in the understanding of this condition and future research directions.
Introduction
Peripartum cardiomyopathy (PPCM) is a rare, idiopathic, and often dilated cardiomyopathy that is marked by systolic dysfunction that presents in late pregnancy or the early postpartum period. A workshop convened by the US National Heart, Lung, and Blood Institute (NHLBI) in the 1990s defined PPCM as heart failure that develops in the last month of pregnancy or up to five months postpartum with left ventricular systolic dysfunction (left ventricular ejection fraction (LVEF) <45% or fractional shortening <30%, or both).12 The rationale for excluding women with heart failure before the final month of pregnancy was to avoid misclassifying pre-existing cardiomyopathies, which typically become symptomatic earlier in pregnancy. However, a large proportion of patients who otherwise meet the criteria for PPCM present before 36 weeks’ gestation,3456 raising concerns that the NHLBI definition may be overly restrictive and lead to the underdiagnosis of PPCM.7 Given this concern, in 2010 the European Society of Cardiology (ESC) defined peripartum cardiomyopathy as heart failure that occurs “towards the end of pregnancy or in the months following delivery, where no other cause of heart failure is found.”7
This review summarizes current literature on the pathogenesis, presentation, and management of PPCM. It is written for both generalists and specialists who care for women with the condition and for investigators studying its pathophysiology and treatment.
Sources and selection criteria
We searched PubMed and Medline for literature on “peripartum cardiomyopathy,” “pregnancy associated cardiomyopathy,” “postpartum heart failure,” and “postpartum cardiomyopathy” from 1 January 2000 to 1 June 2018, along with selected older publications. Preference was given to cohort studies with more than 100 subjects and the few prospective trials performed to date. Only peer reviewed, English language publications were included. We also used relevant guidelines published by the American College of Cardiology Foundation (ACCF), American Heart Association (AHA), and ESC.
Epidemiology and risk factors
Although PPCM occurs worldwide,8 most epidemiologic data come from the United States, South Africa, Nigeria, and Haiti. In the US, its incidence has been estimated at between one in 900 and one in 4000 live births.9101112 A recent study using the US Nationwide Inpatient Sample found that its incidence increased from one in 1181 live births in 2004 to one in 849 live births in 2011 (fig 1).12 Proposed reasons for this increase include rising rates of advanced maternal age, pre-eclampsia, and multiple gestation (driven partly by the use of assisted reproductive technologies), which are risk factors for PPCM; increasing prevalence of cardiovascular risk factors such as hypertension, diabetes, and obesity among women of reproductive age; and the growing recognition of PPCM as a disease entity.1213 Cardiovascular disease has become the leading cause of maternal mortality in the US (25-30% of all maternal deaths), with cardiomyopathy accounting for a half to two thirds of cases.14151617

Temporal trend in the incidence of peripartum cardiomyopathy in the United States. Coloured bars indicate different maternal age groups (see legend). Adapted from Kolte and colleagues.12
{kind=link}
Table 1 summarizes the global incidence of PPCM. Incidence seems to be highest in Nigeria (one in 100 live births)18 and Haiti (one in 300 live births).19 Possible reasons for this include genetic predisposition, a high prevalence of selenium deficiency,26 and, in Haiti, a high prevalence of zinc deficiency27 and pre-eclampsia.1328
Worldwide variation in incidence of peripartum cardiomyopathy
Black women have an increased risk of PPCM.6293031 In two recent US studies, black women accounted for nearly half of cases,1232 even though less than 15% of the US population is black. Incidence is three to four times higher in black women than in white women1033 and lowest in Hispanic women.1230
Maternal age of 30 years or more is a well described independent risk factor for PPCM,6 with an adjusted odds ratio of 1.7-1.8 compared with women less than 30 years.30 In a recent US analysis, the incidence of PPCM was one in 1200 live births among women aged 20-29 years, one in 790 live births among those aged 30-39 years, and one in 270 live births among those aged 40-54 years.12
Pre-eclampsia and eclampsia are associated with PPCM, which, as discussed below, may reflect shared pathophysiology. A 2013 meta-analysis of 22 studies found a 22% prevalence of pre-eclampsia among women with PPCM, more than four times the estimated global prevalence.34 Similarly, of the first 411 women in the EURObservational Research Programme PPCM registry, 22.8% had pre-eclampsia.8 Owing to the heterogeneity of studies performed to date and limitations of data available from Africa and the Caribbean,34 it is unclear whether the association between PPCM and pre-eclampsia differs between black women, who have higher rates of both conditions, and women of other racial and ethnic backgrounds.
A US cohort of 535 women with PPCM identified maternal age of 30 years or more, African ancestry, hypertension, anaemia, substance misuse, asthma, autoimmune disease, and pre-eclampsia or eclampsia as risk factors and found an exponential increase in the risk of PPCM with the presence of each additional risk factor (eg, odds ratio 11 with two risk factors, 795 with six).30 Multiple gestation pregnancy is another well described risk factor.132330 Other reported associations include obesity,23 thyroid dysfunction,29 and prolonged tocolysis.35 Associations with tobacco use1229 and primipara status812 have been inconsistently reported.
Pathogenesis and biology
Although the complete pathogenesis of PPCM remains unclear, recent advances have begun to elucidate the underlying mechanisms. One older hypothesis suggested that PPCM is triggered by viral myocarditis. However, in a series of endomyocardial biopsies performed in 26 patients with PPCM and 33 patients with other cardiomyopathies, the same proportion of specimens in each group (about 30%) had detectable viral genomes.36 In addition, in 38 women from Niger, similar proportions of women with PPCM and controls had serologic evidence of enterovirus infection.37 Inflammation is variably present in endomyocardial biopsies taken from women with the condition, but few patients meet histologic criteria for myocarditis.36383940 Of 40 women in the Investigations in Pregnancy-Associated Cardiomyopathy (IPAC) cohort who underwent cardiac magnetic resonance (CMR) imaging, only one had findings potentially consistent with myocarditis.41 Although inflammatory markers are raised in women with PPCM,4243 the underlying driver does not seem to be infectious.
Current hypotheses
Current thinking favors a “two hit” model of PPCM pathogenesis, whereby a vascular insult caused by antivascular or hormonal effects of late pregnancy and the early postpartum period (fig 2) induces cardiomyopathy in women with an underlying predisposition.
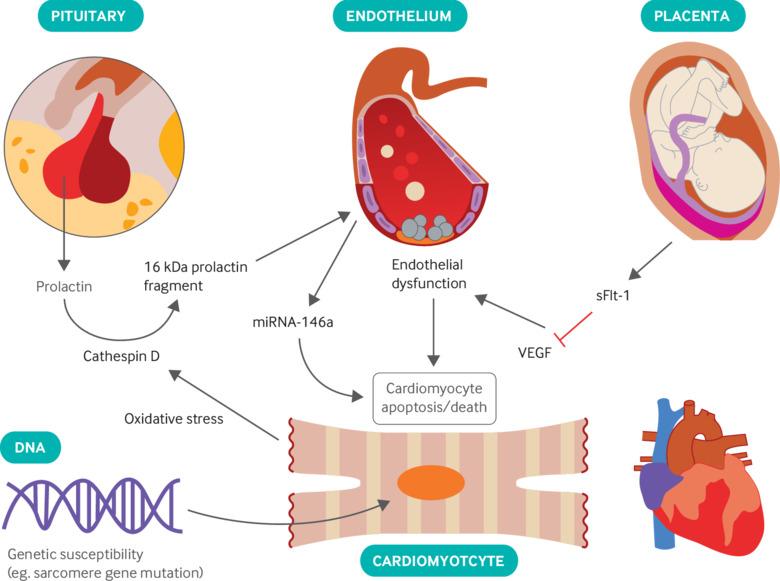
Pathobiology of peripartum cardiomyopathy. Secretion of prolactin by the anterior pituitary gland, upregulation of endothelial microRNA-146a (miRNA-146a), and placental secretion of soluble fms-like tyrosine kinase receptor 1 (sFlt-1) lead to endothelial dysfunction and cardiomyocyte death; genetic susceptibility is also present in some patients. VEGF=vascular endothelial growth factor. See text for details.
{kind=link}
Genetic predisposition: It has long been observed that some cases of PPCM cluster in families.44454647 Analysis of pedigrees affected by the condition and registries of dilated cardiomyopathy (DCM) identified variants in genes that encode the sarcomeric proteins titin, myosin, and troponin.54849 Subsequently, the sequencing of 43 genes associated with DCM in 172 women with PPCM detected 26 truncating variants, 65% of which occurred in TTN, the gene that encodes titin.50 Identifiable variants were present in 15% of women with PPCM, which is similar to the 17% prevalence in women with DCM and significantly higher than that seen in the reference population.50 TTN variants overlapped considerably with mutations known to cause DCM.51 In addition, the presence of a TTN variant compared with variants in other genes predicted lower LVEF at 12 months (LVEF at 12 months 44% v 54% overall, P=0.005; LVEF at 12 months 38% v 52% among black women, P=0.04).50 TTN truncating mutations were seen in 13% of black women and 8% of white women with PPCM, which could be one possible explanation for the worse prognosis seen in black women with the condition. Interestingly, none of the black women with a TTN variant had hypertension or pre-eclampsia, whereas 15 of 17 black women without a TTN variant had hypertension.50 This discrepancy suggests the possibility of a heterogeneous pathophysiology (that hypertensive disease and a certain genetic susceptibility may both cause PPCM through different mechanisms) and merits further study.13 The reasons why some women with these mutations present with PPCM and others present with DCM, which typically manifests later in life and does not spontaneously recover, remain unclear.
Prolactin: A 2007 study suggested that prolactin, a 23 kDa protein secreted by the anterior pituitary, plays a role in the pathogenesis of PPCM.52 It was already known that mice with overexpression of the transcription factor STAT3 (signal transducer and activator of transcription 3) were relatively resistant to anthracycline induced cardiotoxicity owing to upregulation of enzymes such as manganese superoxide dismutase (MnSOD) that scavenge reactive oxygen species (ROS) generated by cardiac metabolism.53 STAT3 is activated in the normal maternal heart during pregnancy and the postpartum period.52 Through unknown mechanisms, oxidative stress stimulates cardiomyocytes to express cathepsin D,54 an enzyme that cleaves prolactin into a 16 kDa fragment, which causes endothelial apoptosis and capillary dropout. Pregnant mice that lacked STAT3 in their cardiomyocytes had increased expression of 16 kDa prolactin. These mice had greater coronary capillary dropout, increased concentrations of ROS, and also exhibited the PPCM phenotype, unlike mice with preserved STAT3 expression. Importantly, administration of bromocriptine to block the secretion of prolactin reversed PPCM in STAT3 deficient mice. The authors also found lower myocardial STAT3 expression (from biopsy and transplant specimens) and higher serum levels of 16 kDa prolactin in small numbers of women with PPCM compared with controls.52 It should be noted that the 16 kDa fragment is just one of several anti-angiogenic “vasoinhibin” molecules derived from prolactin, and that the role of these metabolites has not been investigated to date.55
Subsequent research by the same group showed that 16 kDa prolactin exerts cardiotoxic effects through upregulation of microRNA-146a (miR-146a).5657 The 16 kDa fragment causes endothelial cells to release exosomes containing miR-146a and other microRNAs. MiR-146a blocks several pathways, including Erbb4, Nras, and Notch1, that lead to cardiomyocyte death. Women with PPCM have raised levels of circulating miR-146a, which normalizes after administration of bromocriptine. Administration of antisense oligonucleotides to silence miR-146a decreases the amount of observed systolic dysfunction, capillary dropout, and cardiac fibrosis. Thus, miR-146a may serve as both a biomarker and therapeutic target in PPCM.56
Placental angiogenic factors: The high prevalence of pre-eclampsia in women with PPCM suggests a possible shared pathophysiology. Soluble fms-like tyrosine kinase receptor 1 (sFlt-1) is an anti-angiogenic protein secreted by the placenta in exponentially increasing amounts towards the end of pregnancy. sFlt-1 sequesters circulating vascular endothelial growth factor (VEGF) and placental growth factor (PlGF) and is thought to be the major driver of hypertension and endothelial dysfunction in pre-eclampsia.58 In addition, sFlt-1 levels correlate with global longitudinal strain and increased left ventricular mass in women with pre-eclampsia.5960
A different mouse model suggests that sFlt-1 also contributes to the pathogenesis of PPCM. Proliferator activated receptor gamma coactivator-1α (PGC-1α) is a transcriptional co-activator that promotes angiogenesis and upregulation of MnSOD (thereby mitigating oxidative stress), in addition to regulating mitochondrial metabolism.61 Mice with a cardiac specific genetic deletion of PGC-1α developed dilated cardiomyopathy after pregnancy.62 Administration of exogenous sFlt-1 induced cardiomyopathy and heart failure even in non-pregnant PGC-1α knockout mice and caused discernible but less severe cardiomyopathy in wild-type mice.62 Bromocriptine and VEGF both partially mitigated pregnancy associated cardiomyopathy when administered separately and completely restored cardiac function when administered together.6263
SFlt-1 levels decline rapidly after delivery (after the placental source of sFlt-1 is removed) in healthy women but remain higher than the normal range in women with PPCM.6264 The source of persistently raised sFlt-1 postpartum is not currently known. In the IPAC cohort, the concentration of sFlt-1 at the time of the diagnosis of PPCM correlated with the patient’s New York Heart Association (NYHA) functional class and adverse events.64 It is notable that most women with PPCM present in the postpartum period65; maternal levels of sFlt-1 and other placental hormones peak during labor, and this peak may contribute to a syndrome that manifests postpartum.66 The possible role of other placental hormones, such as activin A, is currently under investigation.6768
Autoimmune mechanisms: Small series have shown that autoantibodies against adrenergic receptors69 and sarcomeric proteins70 are more common in patients with PPCM. However, the clinical significance of these findings is currently unknown.
Clinical presentation and diagnosis
Women with PPCM typically present with symptoms of congestion, including dyspnea on exertion, orthopnea, paroxysmal nocturnal dyspnea, and edema of the lower extremities.6 Less commonly, women present with cardiogenic shock that requires inotropic or mechanical circulatory support. Uncommon presentations include symptomatic or even unstable arrhythmias7172 and arterial thromboembolism.7374 Most women present postpartum, mainly during the first month after delivery; a considerable number present in the late antepartum period; and rare cases present as early as the second trimester.66375 In the IPAC cohort, two women enrolled the day of delivery, and all others enrolled postpartum.76 Black women are diagnosed later postpartum compared with non-black women; it is unclear whether this difference reflects a delay in seeking care, a delay in diagnosis, or a truly different disease presentation (or a combination thereof) in this population.77
Physical examination typically finds evidence of left sided congestion (eg, pulmonary rales) and right sided congestion (eg, raised jugular venous pressure, edema). A left sided or right sided S3 gallop (or both) may be audible, although an S3 gallop can also be present in normal pregnancy. Electrocardiography shows sinus rhythm in most affected women, often with non-specific ST-segment or T-wave abnormalities, or both.78 Chest radiography typically shows pulmonary edema and may show an enlarged cardiac silhouette or pleural effusions (or both). Unlike in normal pregnancy, B-type natriuretic peptide (BNP) and N-terminal pro-BNP are usually raised.79 Troponin may be slightly raised.7580
A diagnosis of PPCM requires echocardiographic evidence of left ventricular dysfunction with LVEF <45% and often (but not always) left ventricular dilatation; presentation peripartum or in the early postpartum period; and absence of an alternative explanation. Echocardiography may also show right ventricular dilatation and dysfunction, pulmonary hypertension, left atrial or biatrial enlargement, functional mitral and tricuspid regurgitation, and intracardiac thrombus.1381
In practice, echocardiography is the most useful form of imaging in PPCM. The lack of exposure to radiation makes echocardiography the ideal imaging modality in pregnant women. CMR imaging may be helpful diagnostically when echocardiography is technically limited.82 Magnetic resonance imaging at 1.5 Tesla is thought to be safe in pregnancy, although guidelines discourage the use of gadolinium, which crosses the placenta and may be teratogenic.8182 Computed tomography imaging has not been studied in PPCM but can rule out other conditions that may present as dyspnea in a peripartum patient, such as pulmonary embolism. In pregnant women, abdominal shielding is recommended to minimize exposure of the fetus to radiation.
Endomyocardial biopsy is generally not indicated, and there are no diagnostic histologic findings. Rare cases in which another cause of heart failure is suspected may merit biopsy when an alternative diagnosis, such as heart block and ventricular tachyarrhythmias suggesting giant cell myocarditis or cardiac sarcoidosis, would change management.
Differential diagnosis
Clinicians must remain vigilant for a diagnosis of PPCM because its symptoms overlap with those of normal pregnancy and it may be missed on initial evaluation (table 2). The differential diagnosis includes pre-existing cardiomyopathy, such as familial dilated cardiomyopathy, previous myocarditis, and drug or toxin induced cardiomyopathy; valvular disease, with mitral stenosis and aortic stenosis being the most common valvular abnormalities to be unmasked by pregnancy; congenital heart disease, such as shunt lesions; and pulmonary arterial hypertension. Because circulating plasma volume and cardiac output increase by 50% by the late second trimester and then plateau for the remainder of pregnancy,83 women with these conditions tend to present with dyspnea and heart failure earlier in pregnancy than do women with PPCM; however, it should be noted that heart failure caused by pre-existing cardiomyopathy or valvular disease can also sometimes present late in pregnany.13 The risk of myocardial infarction, from atherosclerotic plaque rupture or spontaneous coronary artery dissection, is three to four times higher in the peripartum period and, more commonly, the early postpartum period compared with non-pregnant women,84 and it may present with chest pain, dyspnea, heart failure, or a combination thereof.8586 The differential diagnosis also includes pulmonary embolism, the risk of which is five to 10 times higher during pregnancy and the postpartum period,87 and amniotic fluid embolism, a condition marked by shock and respiratory failure during labor or immediately postpartum.
Differential diagnosis of dyspnea in pregnancy*
Natural course and prognosis
Recent data suggest that 50-80% of women with PPCM recover to normal range left ventricular systolic function (LVEF ≥50%), with most of this recovery occurring within the first six months.3767788 These statistics reflect the great improvement in the prognosis of PPCM since the early 1970s, when reported mortality was 30-50% (table 3).899091 This improvement in outcomes probably reflects both the increased recognition of PPCM as a disease entity and advances in the management of heart failure.
Evolution of reported mortality in peripartum cardiomyopathy*
Left ventricular size and ejection fraction at the time of diagnosis most strongly predict left ventricular recovery. In the IPAC cohort, LVEF <30% and left ventricular end diastolic diameter (LVEDD) >6 cm was indicative of decreased likelihood of left ventricular recovery and increased risk of mechanical support, transplant, and death.76 Of 27 women with an initial LVEF <30%, only 10 recovered to a normal LVEF at 12 months, compared with 56 of 65 women with initial LVEF ≥30%. No women with initial LVEF <30% and LVEDD >6 cm recovered systolic function, whereas 50 out of 55 women with LVEF ≥30% and LVEDD <6 cm recovered.76 This finding is consistent with earlier studies from the US9394 and Germany,92 which found that higher LVEF at diagnosis was associated with recovery. In addition, right ventricular function at the time of diagnosis with PPCM independently predicts myocardial recovery and clinical events.95
Black ancestry is associated with a reduced likelihood of recovery. In the IPAC cohort, mean LVEF at 12 month follow-up was 47% for black women and 56% for non-black women (P=0.001), and 16 of 27 black women recovered LVEF ≥50% compared with 50 of 65 non-black women (P=0.13).76 Similarly, in a recent series of 220 women, black women were more likely than non-black women to present with LVEF <30% at diagnosis (56.5% v 39.5%; P=0.03) and were more likely to worsen after diagnosis (35.3% v 18.4%; P=0.02) despite similar use of medication in both groups.77 Although rates of adverse clinical events (such as death and cardiac transplantation) in most contemporary studies are sufficiently low that significant differences between racial groups are not apparent, one recent study of 52 black women and 104 non-black women showed higher rates of death or transplantation in black women (P=0.03).96 Genetic differences probably explain a large proportion of these racial disparities.
PPCM associated with hypertension may represent a different disease phenotype from other cases of PPCM. Studies from Germany,92 Japan,25 and Denmark24 all found higher rates of left ventricular recovery in women who had a hypertensive disorder of pregnancy. In a predominantly black cohort of 39 women in St Louis, Missouri, USA, pre-eclampsia was associated with less left ventricular dilatation at diagnosis and greater recovery in LVEF at one year but, interestingly, also with increased risk of death or readmission for heart failure (P=0.047 for Kaplan-Meier curves).97
In the IPAC cohort, the vasodilatory and pro-angiogenic hormone relaxin was associated with less left ventricular dilatation at diagnosis and earlier recovery of left ventricular function.64 In addition, an increase in troponin concentration is modestly associated with persistent left ventricular dysfunction. In a Chinese series of 106 patients, troponin T ≥0.04 mg/mL had 55% sensitivity and 91% specificity for LVEF ≤50% at six months of follow-up.80
As in other forms of cardiomyopathy, the presence of late gadolinium enhancement (LGE) on CMR signifies fibrosis and may portend decreased recovery of systolic function, although further study of its prognostic value in PPCM is needed.41 Data on CMR findings in PPCM are limited and inconsistent, with LGE reported in 5-71% of women in small series.419899 Of the 40 women In the IPAC cohort who underwent CMR, only two had LGE on baseline assessment, and three had LGE at six months.41 Neither of the two women in this subcohort who died had LGE.41
Complications
Most women with PPCM are diagnosed after presenting with signs and symptoms of heart failure. One study found that 2.6% of women who had PPCM in the US between 2004 and 2011 also had cardiogenic shock.12 Mechanical circulatory support was used in 1.5% of cases, and 0.5% of women underwent cardiac transplantation.12 In the Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS), 48% of women who needed mechanical support for PPCM underwent transplantation within 36 months.100 In the IPAC cohort (n=100), four women underwent left ventricular assist device (LVAD) implantation, one of whom subsequently underwent transplantation.76
Thromboembolism seems to be the most common severe complication of PPCM, affecting 6.6% of women with PPCM in the US12; a similar rate (6.8%) has been reported recently in the EURObservational Research Programme worldwide registry.8 Thrombosis may occur in both left sided and right sided cardiac chambers.7374101102103104105106107108 Mechanisms underlying intracardiac thrombosis in PPCM include cardiac dilatation and hypocontractability leading to blood stasis, as well as endothelial injury.13 In addition, pregnancy is a hypercoagulable state secondary to increased levels of factors VII, VIII, X, fibrinogen, and von Willebrand factor; decreased protein C and S activity; and decreased fibrinolysis—changes that normalize by six to eight weeks postpartum.109110
Arrhythmias contribute greatly to morbidity and mortality in women with PPCM, and sudden death from ventricular tachyarrhythmia is thought to be responsible for more than a quarter of deaths in this population.75111 In the US between 2004 and 2011, 2.1% of women with PPCM had a cardiac arrest, and 2.9% underwent implantation of a cardiac device.12 In a German series of 49 women with PPCM and LVEF, ≤35% of whom used wearable cardioverter defibrillators for 120 days, six patients experienced ventricular tachyarrhythmias; these arrhythmias included five episodes of ventricular fibrillation, two episodes of sustained ventricular tachycardia, and one episode of non-sustained ventricular tachycardia.112 An analysis of 9841 hospital admissions for PPCM in the US found that arrhythmias occurred in 18.7% of cases, with ventricular tachycardia occurring in 4.2%.113
Management of peripartum cardiomyopathy
Because few studies are performed specifically in women with PPCM, management recommendations are generally extrapolated from other forms of heart failure with reduced ejection fraction or derived from expert opinion (or a combination of both). Guidelines advise that standard treatments for heart failure with reduced ejection fraction are indicated in PPCM, with special attention to avoiding adverse fetal effects in women who are still pregnant (table 4).81114115 In our clinical practice, and in accordance with American81 and European116 guidelines, sodium restriction is the mainstay of volume management, and a loop diuretic may be added for symptomatic pulmonary or peripheral edema.117 Care should be taken to avoid over-diuresis during pregnancy, which could result in maternal hypotension and uterine hypoperfusion. If hemodynamics permit, β blockers should be used, with a preference for β1 selective ones (eg, metoprolol tartrate) to avoid stimulating uterine contraction through β2 innervation.613 Angiotensin converting enzyme inhibitors and angiotensin receptor blockers are contraindicated during pregnancy owing to their teratogenicity, which has been reported in numerous studies,118119 but some angiotensin converting enzyme inhibitors are compatible with breast feeding.116 The angiotensin receptor and neprilysin inhibitor sacubitril-valsartan is contraindicated in pregnancy and has not been studied during lactation. Hydralazine and nitrates may be used as vasodilator therapy. On the basis of the RALES and EMPHASIS-HF trials,120121 mineralocorticoid receptor antagonists are indicated in patients with NYHA II-IV heart failure and an LVEF ≤35%114; these agents should be avoided during pregnancy because of their anti-androgenic effects117 but may be used during breast feeding.122 Digoxin may be used safely in pregnancy.123
Safety of drugs for peripartum cardiomyopathy during pregnancy and lactation*
Limited data suggest that the use of β agonists in PPCM may be detrimental. In an observational cohort series of 27 women with PPCM and severe left ventricular dysfunction (LVEF ≤25%), the seven patients who received dobutamine required LVAD or transplantation (or both), whereas 19 of the 20 who did not receive dobutamine improved without advanced cardiac therapies, despite similar reported baseline clinical characteristics.124 By their nature, however, these retrospective data are subject to confounding by indication. Similarly, a recent small German series of five women with PPCM complicated by cardiogenic shock suggested better left ventricular recovery with earlier initiation of mechanical circulatory support.125 Of note, mechanical support allowed for use of lower doses of inotropic agents in this series.
In a mouse model of PPCM with cardiomyocyte specific STAT3 deficiency, administration of isoproterenol, a non-selective β agonist, induced heart failure in STAT3 knockout mice but not wild-type mice, seemingly as a result of decreased glucose uptake and increased oxidative stress in cardiomyocytes of knockout mice.124 These observations, which warrant further study, may argue for preferential use of mechanical circulatory support over positive inotropic agents in women with PPCM and cardiogenic shock as a bridge to recovery (or to durable mechanical support or transplant in those who do not recover).
Levosimendan is a calcium sensitizing agent rather than a catecholamine and may thus lead to superior outcomes when used for inotropic support in PPCM. A retrospective series of 28 patients with cardiogenic shock, including eight women with PPCM, suggested that levosimendan led to rapid improvement in systolic function and hemodynamics in the PPCM subset.126 However, a randomized trial of 24 women with PPCM showed no benefit of levosimendan on LVEF recovery or survival when added to standard treatment for heart failure.127
Thromboembolism is a relatively common complication of PPCM. No published data are available to suggest which women with PPCM warrant anticoagulation.128 However, ESC guidelines advise anticoagulation in patients with PPCM and LVEF ≤35% and in those who have received bromocriptine.115116 AHA guidelines advise considering anticoagulation in women with PPCM and LVEF <30%.81 Other experts have recommended anticoagulation in all women with PPCM until eight weeks postpartum.13 Warfarin crosses the placenta and is teratogenic but is compatible with breast feeding (table 4). The newer directly acting oral anticoagulants are not recommended in pregnancy given the results of animal studies and lack of data in humans. Unfractionated and low molecular weight heparin do not cross the placenta and are considered the anticoagulants of choice for women with PPCM who are still pregnant.
Women with PPCM complicated by arrhythmias may require acute or chronic administration (or both) of antiarrhythmic drugs. Cardioversion and defibrillation are considered safe throughout pregnancy and should be performed without delay in emergencies, as in non-pregnant patients.129 In a non-emergent cardioversion, fetal monitoring may be advisable because of case reports of secondary fetal arrhythmias.75 Despite the limited data on wearable cardioverter defibrillators in PPCM, the ESC and AHA recommend consideration of these devices in women with PPCM and LVEF ≤35% as a bridge to left ventricular recovery or to ICD implantation after three to six months.1381115116117 Because most women will recover, early implantation of an ICD is generally discouraged.116 However, data suggest that ICDs may be underused in women with PPCM who do not recover: in 100 American women, 53 ultimately qualified for implantation of an ICD on the basis of standard device guidelines, but only seven received a device.130
Pregnancy specific considerations
For women who develop PPCM antepartum, a multidisciplinary team comprising obstetrics, anesthesia, and cardiology should individualize patient management, including decisions about the timing and mode of delivery.116131 Given the lack of evidence that early delivery improves maternal or fetal outcomes (in the absence of impending deterioration), women who become stable with medical therapy can continue pregnancy with close monitoring.13 Cesarean delivery should be considered in cases of acute heart failure, according to ESC116 and AHA132 guidelines, but it is otherwise reserved for obstetric indications. Hemodynamic shifts of labor may be mitigated by dense epidural anesthesia and an assisted second stage (use of vacuum or forceps).83
Emerging treatments
Prolactin inhibition
Research implicating prolactin in the pathogenesis of PPCM implies that the inhibition of prolactin might be therapeutic. Bromocriptine and cabergoline are dopamine D2 agonists and inhibit prolactin production, thereby also suppressing lactation.24 Bromocriptine has been associated with thrombotic complications, including myocardial infarction and ischemic stroke,133134 which prompted withdrawal of US approval in 1995 for its use to suppress lactation.13
In an open label randomized trial of 20 South African women with PPCM, women who received bromocriptine experienced greater improvement in LVEF (mean LVEF increased from 27% at baseline to 58% at follow up in the bromocriptine group v 27% to 36% in the control group; P=0.012).135 However, the trial was criticized for its small size and unexpectedly high rates of persistent left ventricular dysfunction and death in the control group.117 In a subsequent observational German registry, 72% of women who “improved” after PPCM had received bromocriptine, compared with 35% of women who did not improve.92
A recent randomized trial of 63 German women with PPCM that compared one week and eight week regimens of bromocriptine found similar improvements in LVEF.136 No women died or required LVAD or transplantation. Notably, two cases of venous thromboembolism and one case of peripheral arterial thrombosis occurred despite the use of prophylactic anticoagulation. No placebo group was included because this was thought to be unethical given the pilot data, but the authors noted that 23 of 37 women with baseline LVEF <30% recovered to an LVEF ≥50% compared with 10 of 27 women with a baseline LVEF <30% in the IPAC cohort (of whom only one received bromocriptine).136 The different racial compositions of the study populations (only one woman was black in the German trial compared with 30 women in IPAC) limits direct comparison of these study outcomes.136 Of note, 72% of women in the IPAC cohort overall recovered to an LVEF ≥50% without the use of bromocriptine.76
Whether prolactin inhibition improves outcomes for all women with PPCM and thus should be part of standard treatment remains controversial. Currently, the addition of bromocriptine to standard treatments for heart failure may be best justified in women with PPCM who have severe cardiomyopathy (LVEF <25%) or cardiogenic shock (or both).116 Breast feeding provides considerable health benefits to the infant and is particularly beneficial in the developing world, where access to clean water and alternative nutrition sources may be limited. Given the benefits of breast feeding and the possibility of thrombotic complications, bromocriptine and cabergoline merit prospective, randomized, placebo controlled evaluation before they are routinely recommended for the treatment of PPCM.
Antisense therapy against microRNA-146a
As noted, in a mouse model of PPCM, administration of antisense oligonucleotides against miR-146a mitigated the development of systolic dysfunction,56 although it did not fully reverse PPCM as seen with bromocriptine in the same mouse model.52 Unlike bromocriptine, however, antisense therapy against miRNA-146 would permit lactation in a nursing mother.13 This treatment has not been tested in humans to date.
VEGF agonism and removal of anti-angiogenic proteins
Apheresis to remove circulating sFlt-1 has been used successfully in women with very preterm pre-eclampsia,137138 and it has been used in a single case report in a woman with severe peripartum cardiomyopathy requiring prolonged biventricular assist device support.139 In a mouse model of PPCM, administration of a VEGF analog mitigated cardiomyopathy.62 VEGF analogs or agonists have not yet been tested in humans.
Serelaxin
Relaxin-2 is a vasodilatory peptide produced by the corpus luteum of the ovary, breast, and placenta that drives many of the cardiovascular adaptations to pregnancy.140 Serelaxin is a recombinant form of relaxin-2 that showed some evidence of benefit in alleviating dyspnea in acute heart failure in the RELAX-AHF trial,141 although it had no effect on mortality from cardiovascular disease (RELAX-AHF-2).142 In a mouse model of PPCM, relaxin increased angiogenesis and cardiomyocyte hypertrophy but did not improve systolic function.143 Further research is needed on the potential benefit of serelaxin.
Perhexiline
Perhexiline is a drug used clinically as an anti-anginal agent that has pleiotropic effects on cardiomyocyte metabolism. Its main effect is to shift metabolism from β oxidation of fatty acids to glycolysis.144 In human studies, perhexiline improved heart failure symptom class145146 and, in one study, systolic function in heart failure with reduced ejection fraction.146 In the previously mentioned study of β agonism in a STAT3 deficient mouse, administration of perhexiline improved left ventricular function and survival in mice treated with isoproterenol.124 Perhexiline has not been studied to date in women with PPCM and is not clinically available in the US owing to concerns about hepatotoxicity and neuropathy.
Pentoxifylline
Pentoxifylline is a xanthine derivative with phosphodiesterase inhibiting and anti-inflammatory properties. Studies have shown evidence of benefit in symptoms and systolic function in heart failure,147 and a meta-analysis of six trials suggested that it reduced mortality.148 In a South African trial, 30 women with PPCM were treated with pentoxifylline and compared with 29 historical controls.149 The composite endpoint of an adverse outcome (NYHA III/IV symptoms, lack of ≥10% improvement in LVEF, or death (or a combination thereof)) occurred in 15 of 29 control patients and eight of 30 women receiving pentoxifylline (P=0.03).149 No subsequent trials of pentoxifylline have been carried out in women with PPCM.
Counseling women with peripartum cardiomyopathy
Breast feeding
The use of pharmacologic prolactin inhibition and cessation of breast feeding are controversial. Some experts and clinical investigators advocate for bromocriptine as part of the management of all women with PPCM,136150 whereas others advise breast feeding for all women who are stable enough to do so, citing fetal benefit and lack of evidence of harm to the mother.13117151 As discussed above, until further data are available, it would be reasonable to consider the use of bromocriptine in women with severe left ventricular dysfunction (eg, LVEF <25%) or cardiogenic shock. Other women with less impaired left ventricular function should be allowed to breast feed if able.
Subsequent pregnancy
Many women who have had PPCM want to become pregnant again. In multiple series documenting subsequent pregnancies after PPCM, LVEF before the subsequent pregnancy is the strongest predictor of outcomes, with worse outcomes among women whose LVEF does not normalize.152 In a review encompassing 191 subsequent pregnancies, women with persistent left ventricular dysfunction (LVEF <50%) had a 50% risk of acute heart failure with worsening cardiomyopathy and, in some subseries from South Africa, a 25-50% risk of mortality.151 Women with normalized LVEF heading into the subsequent pregnancy still had a 20% risk of deteriorating left ventricular function, which persisted long term in 20-50% of women.151 Similarly, a series of 34 women with PPCM from South Africa, Germany, and Scotland found decreased rates of left ventricular recovery and a significantly higher rate of death in women with persistent left ventricular dysfunction heading into a subsequent pregnancy (25% v 0% among women with recovered LVEF, P=0.04).153 In both studies, stillbirth, abortion, and preterm delivery were more common in women with persistent left ventricular dysfunction.151153 Both ESC116 and AHA81 guidelines advise that repeat pregnancy is contraindicated in women with PPCM who have not recovered a normal LVEF.
Currently, no evidence based strategies are available for stratifying risk in women with recovered left ventricular function who wish to conceive again, although some researchers have advocated for the assessment of contractile reserve with stress echocardiography.154155 Women with a history of PPCM should be counseled about the risks of subsequent pregnancy and should be followed closely throughout pregnancy and until six months postpartum with frequent clinical examinations and serial echocardiograms.116151 Although no evidence based monitoring protocols are available, fig 3 summarizes one protocol proposed by Elkayam.151

Recommended schedule of screening echocardiography for women with a history of peripartum cardiomyopathy and subsequent pregnancy. Adapted from Elkayam.151
{kind=link}
Guidelines
Recent relevant society guidelines include the 2013 ACCF/AHA heart failure guidelines,114 the 2016 AHA statement on dilated cardiomyopathies,81 the 2016 ESC practice guideline on severe acute PPCM,115 and the 2018 ESC guidelines on cardiovascular disease in pregnancy.116 These documents make similar recommendations regarding standard medical therapy for heart failure with reduced ejection fraction, anticoagulation, devices, mechanical circulatory support, and multidisciplinary care of the pregnant woman. The most important difference between US and European guidelines is that the European guidelines make a class IIB recommendation for the use of bromocriptine,116 whereas US guidelines consider bromocriptine to be investigational.81 In addition, European guidelines recommend levosimendan as the preferred inotrope in PPCM115116; this drug is not available in the US or Canada.
Knowledge gaps and future directions
Although there have been great advances in the understanding of PPCM during the past decade, many unanswered questions remain (box 1). Key steps in its pathogenesis require further elucidation. A more detailed understanding may allow “sub-phenotyping” of PPCM and enable clinicians to target interventions to specific disease pathways. Except for bromocriptine, no other disease specific treatment for PPCM has emerged to date, and appropriately powered clinical trials of prolactin inhibition and other treatments are needed, especially for patients at highest risk of poor outcomes. Is prolactin inhibition of greater benefit in these women?
Knowledge gaps and future directions in peripartum cardiomyopathy (PPCM) research
Pathogenesis
What factors drive increased expression of the anti-angiogenic hormones (the 16-kDa prolactin fragment and circulating soluble fms-like tyrosine kinase receptor 1) in women with PPCM?
What other hormonal pathways contribute to the pathophysiology of PPCM, and how?
How do vasculo-hormonal insults interact with underlying genetic susceptibility to produce heart failure and cardiomyopathy?
Does PPCM represent one common pathophysiologic process in all affected women or heterogeneous pathophysiologic processes with a common end result of cardiomyopathy?
Diagnosis
Are any biomarkers specific for the diagnosis of peripartum cardiomyopathy (eg, microRNA-146a)?
Can advanced cardiac imaging be used to distinguish PPCM from pre-existing cardiomyopathy?
Management
What is the optimal management of PPCM with severely reduced left ventricular ejection fraction (LVEF) or cardiogenic shock (or both), and how does it differ from the management of other women with PPCM?
Does bromocriptine improve outcomes compared with the standard treatment for heart failure in all or a subset of women?
Can disease specific treatments reverse the pathophysiology of PPCM early in its course to accelerate recovery and prevent long term cardiomyopathy?
Which women with PPCM warrant therapeutic anticoagulation as prophylaxis against thromboembolism?
Which women with PPCM warrant a wearable cardioverter defibrillator as a bridge to myocardial recovery or implantable cardioverter defibrillator?
What is optimal pharmacologic management of PPCM with recovered LVEF?
How can women with PPCM and recovered LVEF be risk stratified for adverse events in a subsequent pregnancy (eg, clinical features, contractile reserve, advanced imaging)?
Should women with PPCM routinely undergo genetic testing? If a woman has an identified gene mutation, should relatives undergo cascade testing? Should relatives undergo routine screening evaluation (such as echocardiography)?
Can pharmacotherapy or other interventions prevent the development of PPCM in women at increased risk?
Another key unanswered question about the management of PPCM (as is the case for other causes of heart failure) is the optimal treatment of women with recovered LVEF, who make up the majority of cases. Although heart failure with recovered ejection fraction generally has a more favorable natural course than heart failure with reduced or preserved ejection fraction,156 patients retain some risk of recurrent heart failure and adverse outcomes.157 Further research is needed to identify appropriate drug withdrawal strategies and to elucidate the benefit, if any, of continued neurohormonal blockade after ejection fraction recovery, for patients with heart failure overall and specifically in PPCM.158 Finally, the genetic susceptibility identified in at least a proportion of women with PPCM raises several additional questions.
Conclusions
Peripartum cardiomyopathy is an uncommon but serious medical condition that affects women throughout the world. While the underlying pathophysiology remains unclear, vasculo-hormonal influences and genetic susceptibility probably play a role. Ongoing efforts at the bench, bedside, and population level that leverage international collaborations, such as the ongoing worldwide PPCM registry, will be needed to answer unresolved questions and define optimal management strategies in PPCM.8 Such collaboration will be crucial to enabling the identification of novel treatments and improving patient outcomes in this potentially life threatening condition.
Glossary
ACCF: American College of Cardiology Foundation
AHA: American Heart Association
BNP: B-type natriuretic peptide
CMR: Cardiac magnetic resonance
DCM: Dilated cardiomyopathy
ECG: Electrocardiography
ESC: European Society of Cardiology
IPAC: Investigations in Pregnancy-Associated Cardiomyopathy
LGE: Late gadolinium enhancement
LVAD: Left ventricular assist device
LVEDD: Left ventricular end diastolic diameter
LVEF: Left ventricular ejection fraction
miR-146a: microRNA-146a
MnSOD: Manganese superoxide dismutase
NHLBI: National Heart, Lung, and Blood Institute
PGC-1α: Proliferator activated receptor gamma coactivator-1α
PPCM: Peripartum cardiomyopathy
ROS: Reactive oxygen species
sFlt-1: Soluble fms-like tyrosine kinase receptor 1
STAT3: Signal transducer and activator of transcription 3
VEGF: Vascular endothelial growth factor
How patients were involved in the creation of this article
We asked a patient advocate of one of the authors (MMG) to review the manuscript. This patient has been active in raising awareness of peripartum cardiomyopathy and heart disease in women by starting a local advocacy group, fundraising for clinical research and patient and family support, and championing national and international initiatives. She highlighted the incomplete understanding of underlying pathophysiology and emphasized the importance of future research in this field. Like many PPCM experts, she cautioned that data to support routine use of bromocriptine is lacking and called for a prospective study to define efficacy and safety. On the basis of her current understanding of genetic predisposition, she also advocated for genetic testing of women with suggestive family history. We included these important points in the manuscript.
Footnotes
Series explanation: State of the Art Reviews are commissioned on the basis of their relevance to academics and specialists in the US and internationally. For this reason they are written predominantly by US authors
Contributors: MCH performed the literature search, organized the review, wrote the draft article, and revised the manuscript. MMG organized the review, contributed to the literature search, edited multiple versions of the manuscript, contributed to all sections of the manuscript, and is the guarantor.
Competing interests: We have read and understood BMJ policy on declaration of interests and declare the following interests: none.
Provenance and peer review: Commissioned; externally peer reviewed.