Article Text

Abstract
Objective To assess the contemporary prevalence of, and factors associated with angina pectoris symptoms, and to examine the relationship to coronary atherosclerosis in a middle-aged, general population.
Methods Data were based on the Swedish CArdioPulmonary bioImage Study (SCAPIS), in which 30 154 individuals were randomly recruited from the general population between 2013 and 2018. Participants that completed the Rose Angina Questionnaire were included and categorised as angina or no angina. Subjects with a valid coronary CT angiography (CCTA) were categorised by degree of coronary atherosclerosis; ≥50% obstruction (obstructive coronary atherosclerosis), <50% obstruction or any atheromatosis (non-obstructive coronary atherosclerosis) or none (no coronary atherosclerosis).
Results The study population consisted of 28 974 questionnaire responders (median age 57.4 years, female 51.6%, hypertension 19.9%, hyperlipidaemia 7.9%, diabetes mellitus 3.7%), of which 1025 (3.5%) fulfilled the criteria of angina. Coronary atherosclerosis was more common in individuals having angina compared with those with no angina (n=24 602, obstructive coronary atherosclerosis 11.8% vs 5.4%, non-obstructive coronary atherosclerosis 38.9% vs 37.0%, no coronary atherosclerosis 49.4% vs 57.7%, all p<0.001). Factors independently associated with angina were birthplace outside of Sweden (OR 2.58 (95% CI 2.10 to 2.92)), low educational level (OR 1.41 (1.10 to 1.79)), unemployment (OR 1.51 (1.27 to 1.81)), poor economic status (OR 1.85 (1.38 to 2.47)), symptoms of depression (OR 1.63 (1.38 to 1.92)) and high degree of stress (OR 2.92 (1.80 to 4.73)).
Conclusion Angina pectoris symptoms are common (3.5%) among middle-aged individuals of the general population of Sweden, though with low association to obstructive coronary atherosclerosis. Sociodemographic and psychological factors are highly associated with angina symptoms, irrespective of degree of coronary atherosclerosis.
- angina pectoris
- computed tomography angiography
- atherosclerosis
- epidemiology
- coronary artery disease
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Angina pectoris has historically been considered a common symptom but is less frequently studied in the past decade.
The correlation between angina pectoris and obstructive coronary artery disease has been found to be low, when invasively investigated in clinical settings.
The association between angina pectoris and obstructive coronary artery disease in the general population is not well studied.
WHAT THIS STUDY ADDS
The novelty of this study is the investigation of angina pectoris symptoms in a large general population sample in combination with evaluation of coronary atherosclerosis at coronary CT angiography (CCTA).
Among middle-aged people from the general population, angina pectoris symptoms are still common (3.5%).
The association between angina pectoris symptoms and coronary atherosclerosis is even weaker in this setting, with only 11.8% having obstructive coronary atherosclerosis at CCTA.
Sociodemographic and psychological factors are highly associated to having angina pectoris symptoms.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Highlights the complexity of assessing angina pectoris symptoms and the need of a holistic approach.
Gives further strength to an initial anatomical investigative approach.
Points to the need of reflection of other cardiac causes of angina pectoris symptoms.
Introduction
The most prevalent form of coronary artery disease (CAD) is its chronic form, chronic coronary syndrome (CCS), of which the most common clinical presentations is angina pectoris, defined as a symptom-based diagnosis of suspected CAD, often verified objectively.1 According to older cross-sectional studies and more recent studies using administrative data, the prevalence of angina appears to be about 2%–7% among middle-aged individuals in developed countries.2–5
Observational studies on angina prevalence are often based on data from either unstructured self-reported diagnosis or administrative data, hence deficient of symptom evaluation. Such studies have obvious biases, and the results must be interpreted carefully. There is a lack of large studies using symptom questionnaires in general population samples and current data on prevalence can therefore be questioned.
The association between a clinical diagnosis of angina and obstructive CAD, defined as epicardial coronary artery stenosis of ≥50%, is weak.1 In studies examining the association between angina and degree of CAD in patients with a clinical indication of invasive coronary angiography, up to 50%–70% have non-obstructive CAD or normal coronary arteries.6–8 There is though no previous large cross-sectional study of unselected individuals from the general population, investigated by coronary angiography.
We hypothesised that in a general population, angina is still common, weakly associated with obstructive CAD and with determinants indicating a heterogeneous aetiology. The aim of this study was to explore the contemporary prevalence of, and factors associated with angina, based on a symptom questionnaire, and its association with degree of coronary atherosclerosis at coronary CT angiography (CCTA) in a large sample of middle-aged individuals, from a western high-income society general population.
Methods
Study design and population
This cross-sectional study is based on data from the Swedish CArdioPulmonary bioImage Study (SCAPIS), an observational study of randomly selected individuals from the general population. Details of the SCAPIS study protocol, recruitment and population have been published elsewhere.9 In summary, 30 154 individuals aged 50–64 years were recruited 2013–2018 at six Swedish university hospitals, using the Swedish population register. The only exclusion criteria were inability to understand written or spoken Swedish for informed consent and lack of a Swedish personal identification number. The study participants in SCAPIS underwent radiological and physiological examinations, as well as blood sampling and an extensive questionnaire, including a variant of the Rose Angina Questionnaire.10 In this variant, a site-map question about location of chest pain was excluded due to technical reasons. In the present study, all participants who completed the Rose Angina Questionnaire were included.
Variables
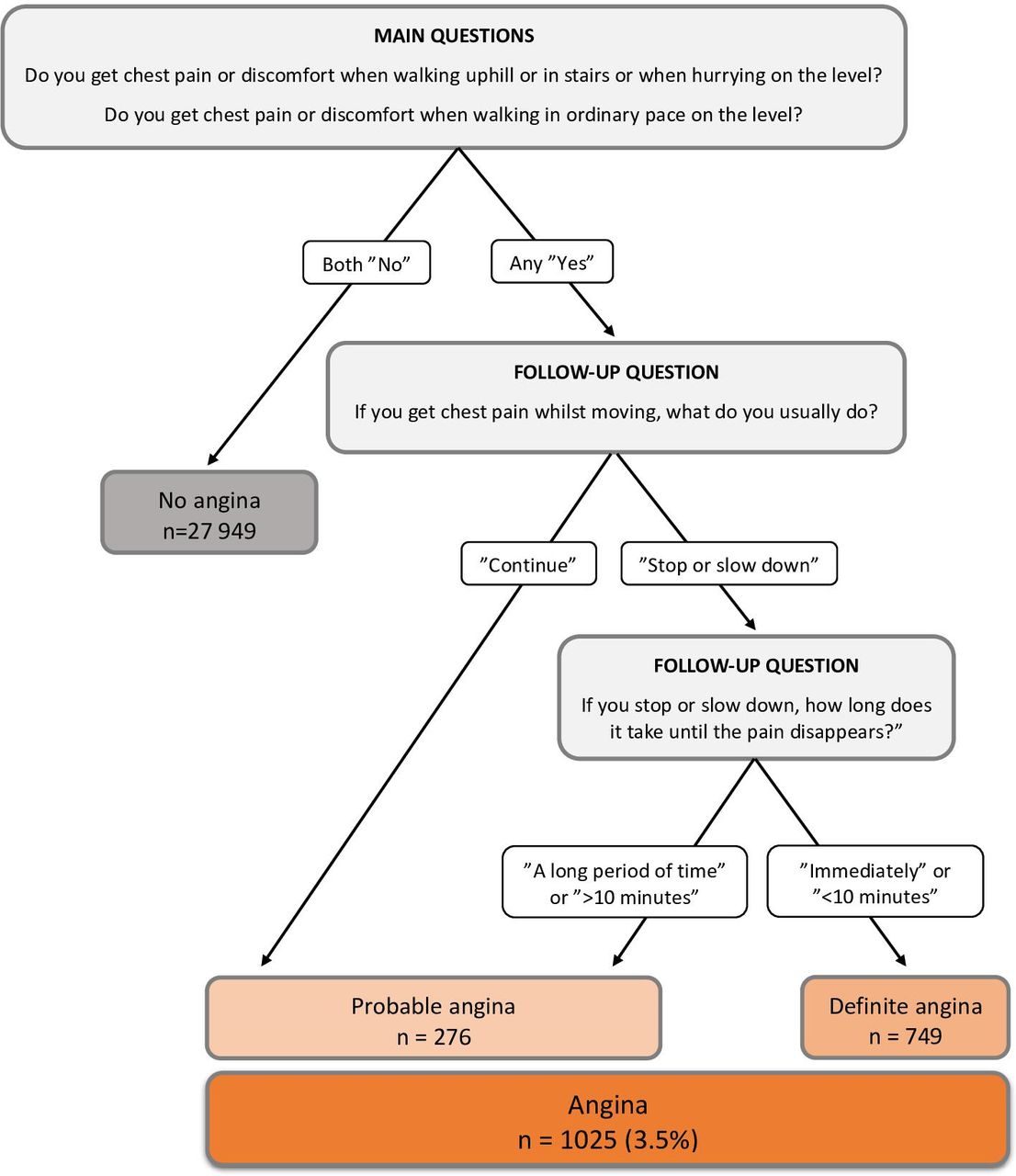
Based on the Rose Angina Questionnaire algorithm, we categorised individuals into the following: (1) No angina; subjects answering ‘no’ to both two main questions: (a) ‘Do you get chest pain or discomfort when walking uphill or in stairs or when hurrying on the level?’ and (b) ‘Do you get chest pain or discomfort when walking in ordinary pace on the level?’ (2) Angina; subjects answering ‘yes’ to any of the two main questions above, in combination with the following answers to the two follow-up questions: (c) ‘If you get chest pain while moving, what do you usually do?’—either ‘slow down’ or ‘stop’ (definite angina), or ‘continue’ (probable angina), and (d) ‘If you stop or slow down, how long does it take until the pain disappears?’—either ‘immediately’ or ‘within 10 min’ (definite angina), or ‘more than 10 min’ or ‘pain duration for a long period of time’ (probable angina).
In SCAPIS, subjects underwent electrocardiogram-gated CT; non-contrast for coronary artery calcification (CAC) imaging followed by administration of beta-blocker (if required) and sublingual glyceryl nitrate before intravenous contrast media for CCTA imaging. Subjects with contraindication to intravenous contrast media were excluded. In our study, subjects having CCTA images with technically non-assessable proximal segments were excluded. Further details of the procedures and how images were read can be found elsewhere.9
According to findings of degree of coronary atherosclerosis at CCTA, we categorised individuals as follows: (1) no coronary atherosclerosis; ‘no findings’ in all 18 segments; (2) non-obstructive coronary atherosclerosis; ‘<50% obstruction’ or ‘not assessable because of calcium artefacts’ in any segment; (3) obstructive coronary atherosclerosis; ‘≥50% obstruction’ in any segment. We categorised CAC score by Agatston Units into 0, 1 to 10 (very low), 11 to 100 (low), 101 to 400 (intermediate), and >400 (high).
From the self-report SCAPIS questionnaire, information on age, sex, civil status, educational level, occupational and economical status, and previous or current diseases were collected, as well as life-style variables, including smoking habits, alcohol consumption and physical activity (Grimby scale).11 Degree of general stress was assessed based on response to ‘Have you experienced a period of stress at work or at home within the last five years’ used in the INTERHEART study.12 Feeling depressed was evaluated based on response to ‘Feeling sad, gloomy or depressed during a two week period (or longer) in the last twelve months’ and categorised as yes or no.12 Activity patterns were obtained from an accelerometer worn for 7 days and categorised as per cent of wear time in sedentary activity or moderate/vigorous activity.13
Data on physical status, including anthropometry (waist circumference, body mass index (BMI), systolic and diastolic blood pressures) and clinical chemistry (plasma total cholesterol, high-density lipoprotein (HDL) cholesterol, triglycerides, calculated low-density lipoprotein cholesterol, glucose, HbA1c, high-sensitivity C reactive protein (hs-CRP) and creatinine) were collected during the initial SCAPIS visit. Estimated glomerular filtration rate was computed in accordance with the CKD-EPI formula.
Statistical methods
SPSS Statistics (V.26) was used for data handling, variable coding and statistical analyses. Statistics were presented as frequency and percentage for categorical variables and mean and SD or median and IQR for continuous variables. Statistical analysis was made using χ2 for categorical variables, independent t-test or one-way analysis of variance in normally distributed continuous variables, and the Mann-Whitney test or Kruskal-Wallis for analyses of continuous variables without normal distribution. To avoid type I error inflation, the Holm-Bonferroni correction for multiple tests was applied. Results were considered statistically significant if corrected p<0.04. To study independent associations, logistic regression models were used, and data presented as adjusted OR with 95% CI. Continuous variables were converted to categorical dummy variables on the nominal scale. Unadjusted analyses of all covariates were made initially, giving ground for clinically and data-driven choices of covariates for adjusted analyses. Three adjustment models were used, with covariates from the following categories of characteristics: Model 1 sociodemographic and psychological (age, sex, civil status, birthplace, educational level, occupational and economical status, self-perceived stress and depression); Model 2 adding lifestyle (smoking habits, alcohol consumption and physical activity); Model 3 adding physical status, clinical chemistry and diseases (BMI, diastolic blood pressure, HDL cholesterol, HbA1c, hs-CRP, estimated glomerular filtration rate, and 11 cardiometabolic and pulmonary diseases). To determine relative importance of each variable in model 3, change in −2 log likelihood when removing the variable was estimated.
Results
Participants
A total of 28 974 participants (median age 57.4 years, female 51.6%, hypertension 19.9%, hyperlipidaemia 7.9%, diabetes 3.7%) had completed the Rose Angina Questionnaire and were included in the study. Out of these, 24 602 participants also had a valid CCTA and were included in the analyses of the association between angina symptoms and degree of coronary atherosclerosis (figure 1).

Study participants. CCTA, coronary CT angiography
Prevalence of angina pectoris symptoms and relation to coronary atherosclerosis
Out of 28 974 subjects, 1025 (3.5%) fulfilled the criteria of having angina according to the Rose Angina Questionnaire (figure 2). Definite angina was more common than probable angina, constituting approximately three-quarters of cases. Among the 24 602 participants with a valid CCTA, 11.8% of angina subjects had obstructive coronary atherosclerosis compared with 5.4% with no angina. The prevalence of non-obstructive coronary atherosclerosis was 38.9% in cases with angina and 37.0% in cases without (figure 3, all p<0.001). The differences in CAC score are presented in figure 4, with higher prevalence of low, intermediate and high scores in angina subjects compared with no angina (all p<0.001).

Rose Angina Questionnaire algorithm and outcome of the study participants, N=28 974.

Degree of coronary atherosclerosis (CA) in study participants with valid CCTA and completed Rose Angina Questionnaire, N=24 602. CCTA, coronary CT angiography.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
CAC score in study participants with valid CCTA and completed Rose Angina Questionnaire, N=24 602. CAC, coronary artery calcification; CCTA, coronary CT angiography.
Factors associated with angina pectoris symptoms
Characteristics of the study participants are presented in table 1. Compared with participants without angina, subjects with angina were more likely to be female, born outside of Sweden, unemployed, living alone, having poor economic status and low level of education. Angina subjects also had a higher degree of general stress and had more often felt depressed. Current smoking, low alcohol consumption and being physically inactive were associated with angina. Individuals with angina also had a higher BMI and waist circumference, higher glucose and HbA1c levels, as well as higher hs-CRP. Finally, current and previous co-morbidities were more common among individuals with angina.
Characteristics of the study participants, Rose Angina Questionnaire completed, N=28 974
In online supplemental table S1, the characteristics of the group with completed Rose Angina Questionnaire and valid CCTA are presented, stratified by degree of coronary atherosclerosis. The differences between subjects with angina and no angina, seen in table 1, were consistent in the 23 233 individuals with either no coronary atherosclerosis or non-obstructive coronary atherosclerosis. In the 1369 individuals with obstructive coronary atherosclerosis, the differences between groups were of similar trend, although in a higher degree non-significant, partly due to the small number of subjects.
Supplemental material
In the adjusted analyses (table 2), born outside of Sweden, low educational level, unemployment, poor economic status, high degree of general stress and depression were associated with angina. These associations remained, although attenuated, when lifestyle factors and co-morbidities were added in models 2 and 3. Further, low alcohol consumption and low physical activity were associated with angina, as well as high HbA1c, high hs-CRP, hypertension, previous myocardial infarction, coronary revascularisation, heart failure, atrial fibrillation, chronic obstructive pulmonary disease and obstructive sleep apnoea syndrome. Similar results were seen when the adjusted analyses were separately performed in the stratified groups presented in online supplemental tables S1 and S2. When determining the relative statistical strength of observed variable associations to angina, sociodemographic and psychological factors appeared to be strongly associated (online supplemental table S3).
Supplemental material
Supplemental material
Association with angina pectoris symptoms, logistic regression analyses—three models, N=28 974
Discussion
In this large randomly selected group of middle-aged individuals from the general population, investigated with both CCTA and the Rose Angina Questionnaire, the prevalence of angina pectoris symptoms was found to be 3.5%. Although coronary atherosclerosis was more common in those with angina symptoms than in those without, the majority (88.2%) of subjects with angina symptoms did not have obstructive coronary atherosclerosis. Irrespective of degree of coronary atherosclerosis, the most important factors associated with angina symptoms were sociodemographic and psychological, and their significance appeared to be only partly mediated by lifestyle or co-morbidities.
The only comparable contemporary prevalence data from another high-income, moderate CVD risk society is from the yearly National Health and Nutrition Examination Survey in the USA, using Rose Angina Questionnaire in combination with self-reported angina, reporting a prevalence of 4.8%–5.2% among middle-aged individuals in 2015–2018.3 In the low CVD risk country of Spain, Alonso et al 4 reported a Rose Angina Questionnaire angina prevalence of 2.6% among 8400 individuals in 2015. Nearly three decades ago, the Northern Sweden MONICA study reported an angina prevalence of 4.2% among 1200 randomly selected middled-aged individuals2 and in a meta-analysis of 74 studies published between 1962–2002, Hemingway et al 5 reported an angina prevalence of 5.7%–6.7%. Hence, our finding of a prevalence of 3.5% could be considered low. Although considering the significant improvements in major cardiovascular risk factors that were observed in northern Sweden MONICA project between 1986 and 2009,14 and the decreased incidence of myocardial infarction in the past decade, an even lower prevalence of angina symptoms could have been expected in this general middle-aged population.
In the ESC guidelines on CCS from 2019,1 an updated version of pre-test probability (PTP) levels was presented, adjusted towards lower rates, based on pooled data from three large chest pain studies showing a mean prevalence of obstructive CAD at 14.9%.15 In our study of a large group from the general population, the prevalence was even lower, with 11.8% of individuals with angina symptoms having ≥50% coronary artery obstruction at CCTA. On the contrary, nearly two out of five individuals with angina symptoms had non-obstructive coronary atherosclerosis, where further assessment should be considered, based on the knowledge of increased risk of major adverse cardiac events in this group, compared with those with normal coronary arteries and especially in cases where myocardial ischaemia is objectified.1 8 16 However, non-obstructive coronary atherosclerosis was common also in asymptomatic individuals (37%), constituting subclinical disease where the prognosis and possible effects of preventive treatment has been less studied. This high prevalence can be compared with the findings of a previous South Korean study of 2133 asymptomatic, middle-aged individuals with low CVD risk, investigated with CCTA in a routine health evaluation setting, with a non-obstructive coronary atherosclerosis prevalence of 11.4%.17
Previous studies on social status, depression and stress have reported an associated elevated risk of acute presentations of CAD.18 19 The INTERHEART study investigated the association between psychosocial risk factors with risk of myocardial infarction in 11 119 cases and 13 648 controls, reporting OR 1.55 (95% CI 1.42 to 1.68) for general stress and OR 1.55 (95% CI 1.42 to 1.69) for depression.13 The association between social status, depression and stress and risk of CCS is though less studied. Our finding that sociodemographic and psychological factors were strongly associated with angina symptoms, independent of degree of coronary atherosclerosis, hence gives further support to the importance of these factors. The fact that the associations found in our study were only marginally attenuated by including previous and present cardiorespiratory diseases and lifestyle factors, such as physical inactivity and low alcohol consumption, suggests that other biological pathways are involved. The association between physical inactivity and angina symptoms could be a case of reversed causality but is more likely explained by physical inactivity being a risk factor for developing atherosclerosis and possible microvascular dysfunction, which have been found to be common in patients with non-obstructive CAD investigated invasively.6 20 Regarding low alcohol consumption, there is a possibility of confounding with low socioeconomic status rather than a direct association to angina symptoms.
Clinical implications
These findings underline that evaluation of anginal symptoms is a common clinical situation with high degree of complexity. The associated sociodemographic factors and several comorbidities highlight the importance of a holistic approach in the patient–doctor consultation when evaluating the symptom of chest pain, deciding on the diagnosis of angina pectoris, and assessing the PTP of obstructive CAD.
The recommendation of CCTA as a first-line investigation in patients with chest pain with low-intermediate PTP was added to the latest CCS guidelines, as a shift of focus toward rule-out of obstructive CAD rather than rule-in.1 These recommendations apply to patients with either typical or atypical angina, as well as non-anginal chest pain and dyspnoea. Our study gives additional support to that approach, given the low degree of association to obstructive coronary atherosclerosis found among the symptomatic study participants, but also highlights the need of broad availability of CCTA.
However, lack of obstructive coronary atherosclerosis should warrant reflection on other cardiac causes of angina known to be common in non-obstructive CAD, such as coronary microvascular disease, epicardial or microvascular spasm.6 20–22
Strengths and Limitations
The major strengths of this study are the size of the cohort recruited from the general population from the whole of Sweden and that nearly all participants underwent CCTA. The study also has several limitations. The age span of the study participants was narrow, why extrapolation of our findings to other age groups should be done with caution. Selection bias is possible and was addressed in the SCAPIS pilot study23 and was later evaluated by Bonander et al 24 finding that the average impact of selection on risk factor distributions at baseline appeared small. Another possible bias is that of self-report, ubiquitous in questionnaire-based research. In our study, this could apply to reported background and lifestyle factors as well as responses to chest pain questions and related behaviour. Rose Angina Questionnaire is a standardised method of measuring angina in general populations, well validated to be predictive of ischaemic heart disease morbidity and mortality, with good reproducibility and widely used in epidemiological studies.25–27 Even so, categorisation of angina could have been more secure with access to symptom assessment by trained clinicians, which was implied in a recent small American study.28 In such a large-scale cohort, this is though difficult to implement. Due to technical reasons, the original site-map question on location of chest pain or discomfort was excluded in the SCAPIS questionnaire. If we had been able to add this question, we would have been able to adhere to the current ESC guideline definition of angina pectoris with possible improvement of specificity. Previous studies investigating the prognostic value of different variants of Rose Angina Questionnaire have though found unaltered ability to predict mortality or new coronary events in variants excluding the site of pain.29 30 It is worthwhile to underline that the Rose Angina Questionnaire is a tool meant to be used in epidemiological settings, and the findings in our study of low association between angina symptoms and obstructive coronary atherosclerosis indicate low utility in daily clinical practice. In our study, there was lack of complete questionnaire data in 1180 subjects (3.8%), which we consider relatively sparse. A separate analysis,with these subjects included is enclosed in online supplemental table S4. Finally, the present study did not include data on functional testing, and we could not differ between angina symptoms with and without objective signs of ischaemia.
Supplemental material
Conclusion
This cross-sectional study of a large sample from the general, middle-aged population in a high-income society concludes that angina pectoris symptoms are still common (3.5%) and that the main associated factors are sociodemographic and psychological. The association between angina symptoms and obstructive coronary atherosclerosis at CCTA is however very low in this setting (~12%). This highlights the complexity of assessing anginal symptoms and gives further strength to an initial anatomical investigative approach but also warrants reflection on other cardiac causes.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Swedish Ethical Review Authority, Diary number 2022-00117-02. The study was conducted in accordance with The Deklaration of Helsinki and participants gave informed consent before taking part in the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors TJ is responsible for the overall content as guarantor. KWS, TJ and PT conceived and designed the study. KWS organised the database, extracted data, performed the statistical analyses and created all tables and figures. All authors interpreted the results and KWS drafted the manuscript. JA, EH, AR-F, SS, PT and TY provided intellectual input, contributed to manuscript revision and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.