Article Text

Abstract
Background Dietary modification is a cornerstone of cardiovascular disease (CVD) prevention. A Mediterranean diet has been associated with a lower risk of CVD but no systematic reviews have evaluated this relationship specifically in women.
Objective To determine the association between higher versus lower adherence to a Mediterranean diet and incident CVD and total mortality in women.
Methods A systematic search of Medline, Embase, CINAHL, Scopus, and Web of Science (2003–21) was performed. Randomised controlled trials and prospective cohort studies with participants without previous CVD were included. Studies were eligible if they reported a Mediterranean diet score and comprised either all female participants or stratified outcomes by sex. The primary outcome was CVD and/or total mortality. A random effects meta-analysis was conducted to calculate pooled hazard ratios (HRs) and confidence intervals (CIs).
Results Sixteen prospective cohort studies were included in the meta-analysis (n=7 22 495 female participants). In women, higher adherence to a Mediterranean diet was associated with a lower CVD incidence (HR 0.76, 95% CI 0.72 to 0.81; I2=39%, p test for heterogeneity=0.07), total mortality (HR 0.77, 95% CI 0.74 to 0.80; I2=21%, p test for heterogeneity=0.28), and coronary heart disease (HR 0.75, 95% CI 0.65 to 0.87; I2=21%, p test for heterogeneity=0.28). Stroke incidence was lower in women with higher Mediterranean diet adherence (HR 0.87, 95% CI 0.76 to 1.01; I2=0%, p test for heterogeneity=0.89), but this result was not statistically significant.
Conclusion This study supports a beneficial effect of the Mediterranean diet on primary prevention of CVD and death in women, and is an important step in enabling sex specific guidelines.
- Risk Factors
- Coronary Artery Disease
- Education, Medical
- Systematic Reviews as Topic
- Epidemiology
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
A Mediterranean diet is a key recommendation for primary prevention of cardiovascular disease (CVD) and death.
But current dietary advice is not sex specific, and many Mediterranean dietary studies lack sex disaggregated analyses.
WHAT THIS STUDY ADDS
This is the first meta-analysis focused on the association between a Mediterranean diet and incident CVD and death, specific to women.
We found that a Mediterranean diet was beneficial in women, with a 24% lower risk of CVD and a 23% lower risk of total mortality.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study highlights the need to include sex specific analysis in research and translate such findings into clinical practice guidelines.
Introduction
Cardiovascular disease (CVD) is the primary cause of mortality in women, accounting for ~35% of all female deaths globally.1 Due to sex disparities in treatment and prognostic outcomes for CVD, there have been international calls for sex specific cardiovascular research.1 A healthy diet is a major factor in CVD prevention. However, most historical cardiovascular diet trials have included predominantly male participants or did not report sex specific analyses.2 3 Moreover, current prevention guidelines lack sex specific recommendations for diet.
The Mediterranean diet has prompted increasing interest due to its association with cardiovascular protection.4–7 This diet is described as high in unprocessed plant foods (wholegrains, vegetables, fruit, legumes, nuts, and extra virgin olive oil), moderate in fish/shellfish and low in red/processed meat, dairy, animal fats, and discretionary foods, with low-to-moderate consumption of wine.7 8 Extra virgin olive oil is preferred as the main source of dietary fat due to its high monounsaturated to saturated fat ratio.7 Several meta-analyses have explored the relationship between the Mediterranean diet and incident CVD and death.9–12 Few have performed sex disaggregated subgroup analyses and no meta-analyses have yet looked at the effect of a Mediterranean diet specifically in women. Individual studies that have performed sex specific analyses have been conflicting. Studies have reported both a beneficial effect of higher Mediterranean diet adherence on CVD outcomes in women, similar to men,13 14 while others have reported a benefit only in men.15 16 Individually, these studies lack power, with a requirement for meta-analyses to demonstrate a more precise measure of treatment effect in women. We therefore performed a systematic review and meta-analysis to evaluate the effect of a Mediterranean diet on incident CVD and total mortality, specifically in women.
Methods
This systematic review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement.17 The protocol was registered with PROSPERO (CRD42022316706).
Search strategy
A systematic search was conducted in November 2021 and updated in November 2022 using Medline, Embase, CINAHL, Scopus, and Web of Science. Studies were included if they were in the English language and published from 2003 to the present. We chose our publication period to align with the Mediterranean diet score (MDS) that was first developed in 1995 by Trichopoulo et al 18 and later updated in 2003.4 We excluded clinical registries and grey literature (eg, conferences, dissertations, supplements and unpublished articles). Reference lists of relevant studies were also reviewed. The search strategy was developed using Boolean operators (AND/OR), medical subject headings (MeSH) and truncations. The full search strategy is described in online supplemental file 1. Authors of studies that did not have available full text were contacted to verify their reference and provide a copy.
Supplemental material
Study selection criteria
The population included women aged ≥18 years without previous clinical or subclinical CVD. We excluded studies that did not explicitly indicate if participants were free from CVD at baseline. The intervention was higher adherence to the Mediterranean diet and the comparator was lower adherence to the Mediterranean diet. This was assessed using an a priori MDS. The first model was the traditional MDS (tMDS) developed by Trichopoulou et al 4 to calculate adherence to the Mediterranean diet.
To be included in the review, studies must have measured Mediterranean diet adherence using the MDS (tMDS or modified versions). Common adaptations of the tMDS include the alternate MDS, relative MDS, and modified MDS.6 15 19 Studies that did not use the tMDS or adaptations were only included if their definition of the MDS included all key components: vegetables, fruits, legumes, nuts, grains/cereals, fish, high intake of monounsaturated fats, and meat and meat products. We excluded studies that referred to only certain components of the Mediterranean diet or had combined the MDS with other lifestyle-related factors.
Higher versus lower adherence levels were based on categories of reported MDS (eg, quintiles, quartiles). Higher Mediterranean diet adherence was defined as the highest category reporting the highest range of MDS. Lower Mediterranean diet adherence was defined as the lowest category reporting the lowest range of MDS.
The primary outcomes included incident CVD and total mortality. Incident CVD was defined as: coronary heart disease (CHD), myocardial infarction, stroke, heart failure, cardiovascular death, major adverse cardiovascular events, major adverse cardiac cerebrovascular events and/or patient reported CVD. Outcomes must have been reported with risk estimates (ie, odds ratio (OR), relative risk (RR) or hazard ratio (HR)) and confidence intervals (CI). Secondary outcomes were CHD and stroke. Randomised controlled trials (RCTs) and prospective cohort studies were included. Studies were included only if they had described the appropriate MDS, reported categorical values according to adherence level to the Mediterranean diet and if they were either female only studies or reported data stratified by sex (online supplemental file 2).
Screening and data extraction
Title and abstract screening and full text screening were undertaken independently by three pairs of investigators (AP and DM, AP and RT, AP and SG). Data extraction was conducted by two authors: one investigator (AP) conducted the data extraction from included studies and another investigator (SG) checked for consistency and any discrepancies. The following information was extracted: name of first author, year of publication and citation; location, study name and study aim; study characteristics (eg, study design, cohort size (number of participants) and percentage of women); participant characteristics (eg, sex, age, cardiovascular risk factors and menopausal status); study duration (period of recruitment and follow-up); details of the exposure assessment (range of score and definition of MDS); outcome(s) (incident CVD, total mortality and, if reported, incidence of new cardiovascular risk factors); effect measures (eg, OR, RR, HR) and covariates included in the final model; and interaction effect analysis by sex. If multiple articles were found using the same cohort, the most recently published article that reported sex specific data and/or other stratified analyses was selected. A Microsoft Excel spreadsheet was used to manage and store the extracted information.
Study quality was assessed by two reviewers independently (AP and SG) using the Cochrane risk of bias tool for RCTs (ROB-1) and the Newcastle-Ottawa Scale (NOS) for cohort studies. The Cochrane risk of bias tool assessed the following domains: random sequence generation, allocation concealment, blinding participants and personnel, selective reporting, blinding outcome assessors and incomplete outcome data.20 21 The NOS quality assessment tool for cohort studies included the following three domains: selection, outcome and comparability. NOS scores were categorised as high quality/low risk of bias (7–9 points), moderate quality/medium risk of bias (4–6 points) and low quality/high risk of bias (0–3 points).22 Disagreements in screening, data extraction and risk of bias were resolved by a third investigator (SZ or LL).
Strategy for data synthesis
A narrative synthesis was conducted for all studies using the DerSimonian and Laird random effects models to calculate summary estimates of HRs.23 All reported risk estimates (HR, RR and OR) from included studies were combined for the highest adherence compared with the lowest adherence to the Mediterranean diet. The event rate was <12%, which is reasonably low for the OR and RR to approximate the HR. Incident CVD or total mortality risk estimates were combined to calculate pooled HRs and 95% CIs. The combined risk estimates were presented using forest plots. Publication bias was evaluated by funnel plots and the Duval and Tweedie trim-and-fill method, and then later confirmed with Egger’s regression test.24 Heterogeneity across studies was assessed using the Q statistic. We used the I 2 test to investigate the proportion of variance in observed outcomes due to variance in the true effects.24 Two sensitivity analyses were conducted to assess whether single studies influenced summary results by (1) excluding a study one at a time and (2) excluding studies with lower quality scores (score of 6).
We performed subgroup analyses according to sex and ethnicity. For ethnicity, studies were grouped into European or non-European descent based on study location, country of birth or self-assigned ethnicity breakdown. For sex, all women included in the systematic review were included in the meta-analysis while data for men were retrieved from the included studies that had stratified data by sex. All analyses were performed using the metafor package from RStudio (V.4.2.0).25
Results
A total of 7173 articles up to November 2022 were identified with 3101 duplicates removed. From title and abstract screening, 3880 articles were excluded and 190 were assessed for full text screening. Of these, 16 were included in the meta-analysis, with exclusions shown in figure 1.

Flowchart of the included studies; 16 studies were included in the meta-analysis. 1Other sources included search updates from databases and reference lists.
Description of included studies
The 16 articles were published between 2006 and 2021. All included studies were prospective cohort studies and involved a total of 722 495 female participants, with a median follow-up of 12.5 years (IQR 10.4–14.5). The studies were mainly conducted in the US (n=6)6 14 26–29 and Europe (n=7).15 16 19 30–33 tMDS was used in three studies,30 32 34 10 used derivatives6 13–16 19 27–29 33 while three studies relied on separate definitions.26 31 35 Of the 16 articles, two studies reported total mortality as the only outcome,32 33 four studies reported both incident CVD and total mortality13 14 27 29 and 10 studies reported only incident CVD.6 15 16 19 26 28 30 31 34 35 Study characteristics are summarised in online supplemental file 3.
The quality assessment results are shown in online supplemental file 4. NOS scores ranged from 6 to 8, indicating moderate-to-high quality, with six studies of moderate quality/medium risk of bias6 14 19 26 34 35 and 10 studies of high quality/low risk of bias.13 15 16 27–33
Outcomes and meta-analysis
From the 14 studies that reported CVD events, the crude CVD event rate was 4.02% (27 268 cardiovascular events out of 678 372 female participants). The meta-analysis demonstrated that in female participants, higher Mediterranean diet adherence correlated with lower incident CVD and total mortality. For incident CVD, the pooled HR was 0.76 for the highest versus the lowest category of Mediterranean diet adherence (95% CI 0.72 to 0.81; I2=38.6%, p test for heterogeneity=0.07) (figure 2).

Forest plot of pooled hazard ratios (HRs) in female participants for incident cardiovascular disease (CVD) according to highest versus lowest category of Mediterranean diet adherence using the random effects model. Higher adherence to a Mediterranean diet had a favourable effect on incident CVD (HR 0.76, 95% CI 0.72 to 0.81; I2=38.6%, p test for heterogeneity=0.07). RE, random effects.
For total mortality based on six studies, the pooled HR was 0.77 for female participants in the highest versus the lowest category of Mediterranean diet adherence (95% CI 0.74 to 0.80; I2=20.9%, p test for heterogeneity=0.28) (figure 3).

Forest plot of pooled hazard ratios (HRs) in female participants for total mortality according to highest versus lowest category of Mediterranean diet adherence using the random effects model. Higher adherence to a Mediterranean diet had a favourable effect on total mortality (HR 0.77, 95% CI 0.74 to 0.80; I2=20.9%, p test for heterogeneity=0.28). N/R, not reported; RE, random effects.
Four studies reported CHD, with pooled HRs of 0.75 for the highest versus the lowest Mediterranean diet adherence (95% CI 0.65 to 0.87; I2=20.9%, p test for heterogeneity=0.28). Three studies reported stroke, with no significant association between the highest versus the lowest Mediterranean diet adherence and risk of stroke (HR 0.87, 95% CI 0.76 to 1.01; I2=0.0%, p test for heterogeneity=0.89) observed.
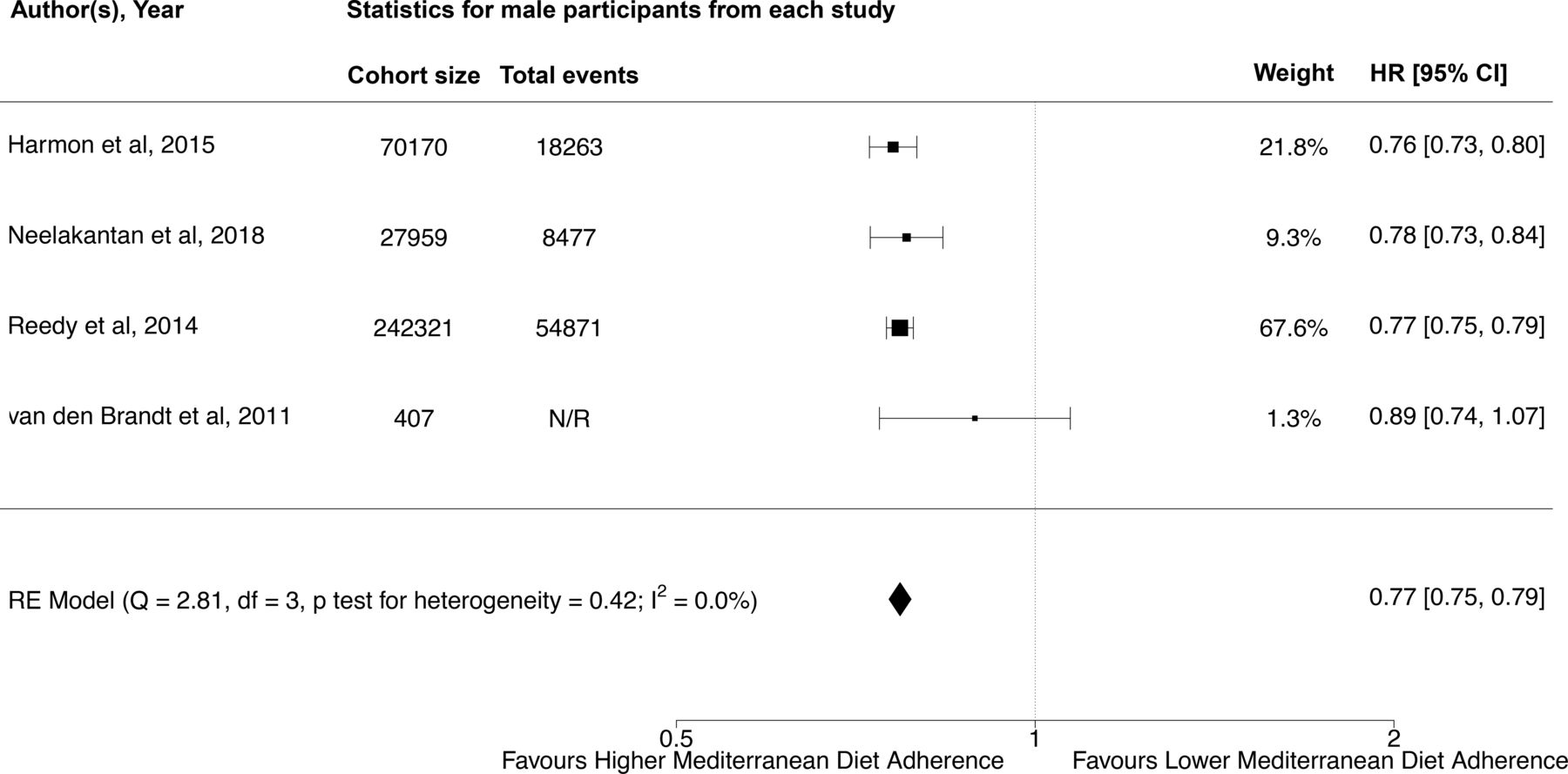
In subgroup analyses by sex, the pooled HRs for the highest versus the lowest Mediterranean diet adherence in men was 0.78 for incident CVD (eight studies; 95% CI 0.72 to 0.83; I2=35.1%, p test for heterogeneity=0.15) and 0.77 for total mortality (four studies; 95% CI 0.75 to 0.79; I2=0.0%, p test for heterogeneity=0.42) (figures 4 and 5). In subgroup analyses of female participants by ethnicity, higher Mediterranean diet adherence was associated with incident CVD for both European (five studies; HR 0.76, 95% CI 0.59 to 0.98; I2=59.4%, p test for heterogeneity=0.04) and non-European descent groups (five studies; HR 0.79, 95% CI 0.72 to 0.87; I2=0.0%, p test for heterogeneity=0.54) (online supplemental file 5 figure S1 and S2).

Forest plot of pooled hazard ratios (HRs) in male participants of incident cardiovascular disease (CVD) for highest versus lowest category of Mediterranean diet adherence using the random effects model. Higher adherence to a Mediterranean diet had a favourable effect on total mortality (HR 0.78, 95% CI 0.72 to 0.83; I2=35.1%, p test for heterogeneity=0.15). RE, random effects.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of pooled hazard ratios (HRs) in male participants of total mortality for highest versus lowest category of Mediterranean diet adherence using the random effects model. Higher adherence to a Mediterranean diet had a favourable effect on total mortality (HR 0.77, 95% CI 0.75 to 0.79; I2=0.0%, p test for heterogeneity=0.42). N/R, not reported; RE, random effects.
The funnel plot indicated signs of publication bias due to asymmetry for incident CVD, although it remained symmetric for total mortality (online supplemental file 6 figure S3 and S4). However, Egger’s test for incident CVD and total mortality were 0.55 and 0.93, respectively, indicating that there was no publication bias.
Our sensitivity analysis demonstrated that no single study had a material effect on the pooled HRs. Excluding one study at a time, the pooled HRs for the highest versus the lowest Mediterranean diet adherence ranged from 0.76 (95% CI 0.72 to 0.80) to 0.83 (95% CI 0.70 to 0.98) for incident CVD and from 0.77 (95% CI 0.75 to 0.80) to 0.77 (95% CI 0.74 to 0.81) for total mortality for women. Excluding studies with a lower quality score (<6), the pooled HRs for the highest versus the lowest Mediterranean diet adherence remained significant for incident CVD (HR 0.77, 95% CI 0.69 to 0.87; I2=56.5%, p test for heterogeneity=0.02) and total mortality (HR 0.77, 95% CI 0.75 to 0.80; I2=16.1%, p-test for heterogeneity=0.31).
Discussion
In this meta-analysis of 16 prospective cohort studies, women with a high adherence versus a low adherence to a Mediterranean diet had a 24% lower risk of CVD and a 23% lower risk of total mortality. To our knowledge, this is the first systematic review to examine the association between Mediterranean diet adherence and CVD and total mortality specifically in women.
The Mediterranean diet is widely known for its protective role against CVD and death.4–6 The PREDIMED (Prevención con Dieta Mediterránea) trial was the largest multicentre RCT to investigate the impact of a Mediterranean diet on cardiovascular outcomes.36 PREDIMED found that participants following a Mediterranean diet supplemented with extra virgin olive oil or nuts had a 31% reduction in cardiovascular event risk compared with controls.36 Unfortunately, the results were not disaggregated according to sex. While multiple systematic reviews have been published on the effect of the Mediterranean diet on CVD and death, no meta-analyses have centred on women. This first meta-analysis of female only studies, or studies that performed sex disaggregated analysis, found that a Mediterranean diet is equally beneficial in women as it is in men, with a 24% lower hazard of CVD (I2=38.6%) and 23% lower hazard of total mortality (I2=20.9%). We were unable to demonstrate a benefit of stroke reduction in women, but this was likely due to the smaller number of studies reporting this secondary outcome.
The inverse association seen in women in the current study is comparable with previous non-sex specific meta-analyses.9 11 12 37–39 For incident CVD, previous meta-analyses found a lower risk, ranging from 10% to 35%, with similar degrees of heterogeneity (I2=36–38%).11 12 37 38 Studies on stroke reported a lower risk of 24–35% and higher heterogeneity (I2=52–69%).11 12 37 39 For total mortality, other meta-analyses found a modest lower risk of 9–10%, with moderate-to-high heterogeneity (I2=49–81%).9 38 Previous reviews that performed subgroup analyses often found a small magnitude of decreased risk for women9 12 but were limited by significant heterogeneity (I2=81.1–86%) and smaller numbers of female participants.9 12 In the current meta-analysis, we included more than 7 00 000 women with a strong association found for the beneficial effect of higher Mediterranean diet adherence on CVD and death. Exclusion of each observational study one at a time in our sensitivity analysis did not substantially influence the pooled HRs, further supporting a strong inverse relationship for incident CVD and total mortality with higher Mediterranean diet adherence in women.
Our subgroup analyses found that the benefit of a Mediterranean diet on CVD persisted in women of both European (lower risk of 24%) and non-European (Asian, Native Hawaiian and African American) descent, with a lower risk of 21%. Our findings are consistent with previous non-sex disaggregated studies whereby a Mediterranean diet was beneficial across different ethnicities, with a slightly higher benefit in Mediterranean countries.10 12 However, this difference may reflect the smaller number of non-European studies that have been published.10 12
Various mechanistic pathways have been shown to influence the lowering effects of the Mediterranean diet on cardiovascular outcomes, including its antioxidant and microbiome effects that are closely associated with the interaction between inflammation and cardiovascular risk factors.40–42 Furthermore, the different components of the Mediterranean diet may contribute to a better cardiovascular risk profile; for example, polyphenols,43 nitrates,44 omega-3 fats, increased fibre from plant foods42 and reduced glycaemic load.45 However, mechanisms explaining the sex specific effect of the Mediterranean diet on CVD and death remain unclear.
This study demonstrated a higher magnitude of decreased risk for CVD in women compared with previous meta-analyses that included both men and women. This could be due to the large sample size of female specific data included in our meta-analysis, resulting in an analysis of a more diverse group of women from different age groups and with varied cardiovascular risk profiles. However, it adds to the need for sex specific research. Female specific cardiovascular risk factors, including premature menopause, pre-eclampsia and gestational diabetes, or female predominant risk factors, such as systemic lupus, can all independently increase CVD risk.46 Common forms of CVD (eg, myocardial infarction) can also have different aetiologies in women compared with men.47 It is possible that preventative measures, such as a Mediterranean diet, that targets inflammation and CVD risk factors, impose differing effects in women compared with men.
Limitations
Our study has several imitations. Firstly, the included studies were observational in nature, with reliance on self-reported food frequency questionnaires to determine exposure and resulting susceptibility to bias. Secondly, studies without sex disaggregated analyses were excluded and individual participant data were not available. Contacting authors to provide individual participant data was considered. This was abandoned as it was deemed unfeasible due to the vast number of studies without sex disaggregated data (n=66) and low response rate, many of which were published more than a decade ago and for which individual participant data were unlikely to be available. However, the large number of studies without sex specific analyses reinforces the importance of our systematic review. Thirdly, adjustments for important confounders, such as cardiovascular risk factors, varied across studies, with subsequent bias towards a more favourable result. Finally, the study was limited by varying definitions of MDS, range of the score and different cut-offs of MDS, which may have contributed to study heterogeneity. This limitation was minimised by including only studies that reported key Mediterranean dietary components. However, the results should be taken with a certain degree of caution considering these limitations and the nature of cohort studies.
Future implications
Our study demonstrates the need for dietary cardiovascular studies to report sex disaggregated analyses. Future research might consider adding more studies that look at the dietary impact on stroke, and subgroup analyses that address female specific cardiovascular risk factors, menopausal status and ethnicity, as well as individual participant data meta-analyses.48
Conclusion
Our systematic review and meta-analysis demonstrated a protective association between higher versus lower adherence to a Mediterranean diet on CVD incidence and total mortality, specific to women. Future research should adopt more sex aggregated research designs to develop tailored dietary guidelines for CVD prevention.
Supplemental material
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @simoneMarschne1, @MMamas1973, @clara_chow, @DrSarahjZaman
Contributors AP was responsible for conducting the systematic review and meta-analysis, and writing the manuscript. SG, DM and RT assisted in the screening stage of the systematic review. SG assisted in data extraction and risk assessment. SM helped perform the statistical analysis. All authors critically reviewed the manuscript. SZ is responsible for the study design, conception of the study, and critically reviewing the manuscript. SZ is responsible for the overall content as the guarantor. SZ accepts full responsibility for the work and the conduct of the study, had access to the data, and controlled the decision to publish.
Funding No funding was received for this study. SZ was supported by a Heart Foundation Future Leader Fellowship (ID 102627) for their work.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.