Alcohol related disorders among elite male football players in Sweden: nationwide cohort study
BMJ 2022; 379 doi: https://doi.org/10.1136/bmj-2022-074093 (Published 21 December 2022) Cite this as: BMJ 2022;379:e074093Linked Editorial
Alcohol related harms and elite men’s football

- Peter Ueda, assistant professor1,
- Björn Pasternak, principal researcher1 2,
- Henrik Svanström, statistician1 2,
- Carl-Emil Lim, doctoral student1,
- Martin Neovius, professor1,
- Magnus Forssblad, orthopaedic surgeon3 4,
- Jonas F Ludvigsson, professor5 6,
- Manzur Kader, postdoctoral researcher1
- 1Clinical Epidemiology Division, Department of Medicine, Solna, Karolinska Institutet, Stockholm, Sweden
- 2Department of Epidemiology Research, Statens Serum Institut, Copenhagen, Denmark
- 3Department of Molecular Medicine and Surgery, Stockholm Sports Trauma Research Center, Karolinska Institutet, Stockholm, Sweden
- 4Ortopedi Stockholm, Stockholm, Sweden
- 5Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Solna, Sweden
- 6Department of Paediatrics, Örebro University Hospital, Örebro, Sweden
- Correspondence to: P Ueda peter.ueda{at}ki.se
- Accepted 26 November 2022
Abstract
Objectives To assess whether male elite football players are at increased risk of alcohol related disorders compared with men from the general population, and whether such an increased risk would vary on the basis of calendar year of the first playing season in the top tier of competition, age, career length, and goal scoring abilities.
Design Nationwide cohort study.
Setting Sweden, 1924-2020.
Participants 6007 male football players who had played in the Swedish top division, Allsvenskan, from 1924 to 2019 and 56 168 men from the general population matched to players based on age and region of residence.
Main outcome measures Primary outcome was alcohol related disorders (diagnoses recorded in death certificates, during hospital admissions and outpatient visits, or use of prescription drugs for alcohol addiction); secondary outcome was disorders related to misuse of other drugs.
Results During follow-up up to 31 December 2020, 257 (4.3%) football players and 3528 (6.3%) men from the general population received diagnoses of alcohol related disorders. In analyses accounting for age, region of residence, and calendar time, risk of alcohol related disorders was lower among football players than among men from the general population (hazard ratio 0.71, 95% confidence interval 0.62 to 0.81). A reduced risk of alcohol related disorders was observed for football players who played their first season in the top tier in the early 1960s and later, while no significant difference versus men from the general population was seen in the risk for football players from earlier eras. The hazard ratio was lowest at around age 35 years, and then increased with age; at around age 75 years, football players had a higher risk of alcohol related disorders than men from the general population. No significant association was seen between goal scoring, number of games, and seasons played in the top tier and the risk of alcohol related disorders. Risk of disorders related to other drug misuse was significantly lower among football players than the general population (hazard ratio 0.22, 95% confidence interval 0.15 to 0.34).
Conclusions In this nationwide cohort study, male football players who had played in the Swedish top tier of competition had a significantly lower risk of alcohol related disorders than men from the general population.
Introduction
The relation between football and alcohol is a complex one, both on and off the field. Alcoholic beverages are frequently consumed by fans during football games and alcohol companies sponsor major football teams and tournaments.123 Drinking has also been common among football players, and numerous players (including some of the finest in history), have had alcohol addiction during and after their careers.4
Giuseppe Meazza, of Inter Milan and the Italian national team that won the 1934 and 1938 World Cups, was known for his nightly drinking, often arriving late and hungover to practice and games.5 Ferenc Puskas, the forward who led Hungary’s so-called Golden Team of the early 1950s, is said to have known only two words in English, one of which was “vhisky.”6 George Best, of Manchester United and Northern Ireland, had a well documented addiction, having described giving up alcohol in 1969 as the “hardest 20 minutes of my life.”7 During and after his career, Best was repeatedly arrested for alcohol related incidents, had alcoholic cirrhosis, and received a liver transplant—although he continued to drink and died at age 59 years.8 Garrincha, a goal scoring winger who helped Brazil win successive World Cups in 1958 and 1962, is said to have consumed one bottle of cachaça each day in his adult life and died of alcoholic cirrhosis at age 49 years.9 Diego Armando Maradona, of Napoli and Argentina, had a widely publicised cocaine and alcohol addiction.10 More recently, the England international Wayne Rooney revealed that he was binge drinking for days to cope with the pressure to perform during his career.11
Studying alcohol related disorders among elite football players is important for several reasons. Elite football players face many psychosocial stressors, including the constant pressure to perform at a high level, public attention and fame, and the risk of being injured, dropped from the team, and outcompeted by other players; such stressors, among others, have been suggested to increase the risk of alcohol related disorders.121314 The period of transitioning out of elite sports can be challenging, and retirement from elite sports has been linked with mental health problems and alcohol related disorders.14151617 Moreover, a football related drinking culture affecting both players and fans has been highlighted as a potential public health concern.1234 Data on the epidemiology of alcohol related disorders among elite football players could inform the need for psychosocial support and prevention of such disorders among elite football players and the discussion regarding the association between football, alcohol, and public health.
In Sweden, similar to many other countries, alcohol consumption has been deeply ingrained in football culture for both players and fans.18 In this study, we used a nationwide cohort of male football players in the top tier of competition in Sweden and nationwide register data to assess whether elite football players were at increased risk of alcohol related disorders compared with men from the general population. In secondary analyses, we assessed disorders related to other drug misuse among football players versus men from the general population.
Methods
Data sources
Detailed information about the data sources and the methods used to construct the study cohort are provided in the supplementary material. Information about football players was collected from data sources of all current and former football players in the Swedish top tier of competition, Allsvenskan, and was compiled by the Swedish Association of Football Historians and Statisticians. These data comprised the full name, birth date, seasons and number of games played, number of goals scored, teams represented and player position (outfield or goalkeeper). In databases run by the Swedish Tax Agency and the Federation of Swedish Genealogical Societies, the name and birth date were used to search for the player’s personal identity number, a number given to all inhabitants in Sweden which enables linkage of individual level data across data sources (supplementary material and supplementary table 1). We used several nationwide health and administrative registers, including the Total Population Register (vital status, region of residence, region of birth), Patient Register (outcomes), Cause of Death Register (outcomes), Prescribed Drug Register (outcomes), Statistics Sweden (income, education), and Swedish Military Conscription Register (results from psychological and physical tests at military conscription).
Study population
A flowchart for the study population is shown in supplementary figure 1. All football players who had played at least one game in Allsvenskan from its first season in 1924 to 2019 were included. We excluded players whose personal identity number were not available in the databases (eg, because players had removed themselves from public databases, had died before the introduction of identity numbers, or were foreign players without an identity number). We also excluded players for whom a personal identity number could not be identified because of multiple individuals having the same name and birth date, and it was not possible to identify the football player among them. We excluded players who were not registered in the Total Population Register, which started in 1969.
Each football player was matched in a 1:10 ratio with men from the general population, based on year of birth, region of residence, and vital status, to form a base cohort. The matching variables had no missing data. The matching date was 1 January in the year when the football player played his first game in Allsvenskan or was first registered as a resident in Sweden (if this occurred after the first year of play in Allsvenskan), and matching was performed using the Total Population Register. For players who played their first season before 1969 (ie, the start of the Total Population Register), we selected men from the general population matched by vital status and region of residence on 1 January 1969. The date when players and men from the general population were matched constituted cohort entry.
From the base cohort, we excluded players (and matched men from the general population) and men from the general population who were not born in Sweden and who had their first date of residence in the country after age 15 years. We used this exclusion criterion because foreign players are likely to emigrate during or shortly after their football career, which would preclude long term follow-up.
Outcomes
The primary outcome was alcohol related disorders recorded in the Cause of Death Register (primary or contributing causes of death), National Patient Register (primary or secondary diagnosis during hospital or outpatient visits), or Prescribed Drug Register (filled prescriptions for drugs used to treat alcoholism). The secondary outcome was disorders related to misuse of other drugs. The ICD-8, ICD-9, ICD-10 (international classification of diseases, 8-10th revisions) codes and Anatomical Therapeutic Chemical codes used for the definition of the outcomes are shown in supplementary table 2.
Statistical analysis
Football players and men from the general population were followed from cohort entry to emigration, outcome event, death, or end of follow-up (31 December 2020). Emigration, death that did not include an outcome event, and end of follow-up constituted censoring events. We used Cox regression analysis with age as the time scale and adjusted for region of residence, place of birth, and calendar time as a time varying covariate (supplementary table 3) to estimate the hazard ratio for the risk of the primary outcome among football players versus men from the general population.
We performed additional analyses. Rules and norms regarding alcohol consumption among football players have differed substantially over time in Sweden.1819 We therefore modelled the interaction between the year of the player’s first season in the top tier of competition using restricted cubic splines with 3 knots and a flexible parametric survival model20 to calculate the hazard ratio for football players versus matched men from the general population by year of the football player’s first season.
Some of the most high profile cases of alcohol addiction have occurred among players famous for their goal scoring abilities. Previous studies have shown associations between personality traits and alcohol consumption.21 Therefore, we hypothesised that factors potentially associated with scoring goals (eg, sensation seeking),21 might also be associated with the risk of alcohol related disorders. Further, football players who have played many games and seasons in the top tier could have been more exposed to drinking culture associated with elite football, fame, and public scrutiny. Another possibility is that football players with drinking problems could have terminated their careers early. We therefore hypothesised that the number of games and seasons in the top tier might be associated with alcohol related disorders.
In analyses restricted to football players, we used the Cox regression model additionally adjusted for birth cohort (categorical variable; supplementary table 3) to separately assess the association with alcohol related disorders for number of goals scored per 10 games (among outfield players who had played at least 10 games), the number of top tier games played, and the number of seasons played, modelled using cubic splines with 3 knots. We also assessed the risk of alcohol related disorders among outfield players versus goalkeepers.
Studies have indicated that elite athletes could be at increased risk of alcohol related disorders after retirement from their elite careers141522 owing to changes in life circumstances associated with retirement. We therefore assessed whether the risk of alcohol related disorders among football players versus men from the general population varied across age. As outcome data from death certificates and hospital admissions might poorly reflect the timing of the first diagnosis, we set the earliest cohort entry to 1 January 2002, one year after the start of nationwide coverage for outpatient visits in the National Patient Register. We excluded football players (and matched men from the general population) and men from the general population who had died, emigrated, or had any history of alcohol related disorders before cohort entry. We calculated the hazard ratio of the risk of alcohol related disorders for football players versus men from the general population using the total follow-up time in this analysis, and in another analysis modelling age using restricted cubic splines with 3 knots.
We performed a sensitivity analysis. The earliest possible cohort entry was in 1969. If players and men from the general population had different risks of death with alcohol related disorders, the exclusion of those who died before 1969 could introduce left truncation bias owing to a depletion of individuals susceptible to alcohol related disorders.23 We therefore conducted an analysis including only those players and those men from the general population who were 49 years or younger at cohort entry.
We performed exploratory analyses assessing the impact of accounting for some characteristics that might differ between elite football players and men from the general population. Some men from the general population could have had severe health or social problems that precluded participation in the workforce and increased the risk of alcohol related disorders. Therefore, we performed two analyses that excluded men from the general population with zero registered income at cohort entry, and at age 40-44 years (supplementary table 4). For these analyses, we excluded men from the general population without available income data and football players with no matched men from the general population for whom income data was available. We then performed the analysis with and without exclusion of men from the general population with zero registered income.
Next, we used data from the Military Conscription Register. Firstly, we performed the analysis including all football players and men from the general population born in 1951-87, because military conscription was mandatory at around age 18 years for men born during this period.24 Individuals living abroad, those with certain health conditions, and those with functional impairments were exempt from conscription or tests (supplementary material (data sources) and supplementary table 4), so we performed the analyses excluding football players and men from the general population born 1951-87 without complete data on test results, including stress reliance, cognitive ability, body mass index, muscle strength, and cardiorespiratory exercise capacity (supplementary table 4). We then performed analyses adjusting for stress resilience and cognitive ability scores.252627 Finally, we further adjusted the model for body mass index, muscle strength, and cardiorespiratory exercise capacity.
The secondary outcome of disorders related to other drug misuse was also assessed. ICD-8 codes, which were used before 1987, did not contain diagnoses suitable for capturing the secondary outcome in death certificates, so we set the earliest date of cohort entry to 1 January 1987, when nationwide coverage in the National Patient Register for inpatient diagnoses began. In these analyses, we excluded players who died or emigrated before 1987 and their matched men from the general population, and men from the general population who died or emigrated before 1987. We also excluded players and men from the general population aged 65 years or older in 1987 to avoid potential left truncation bias.23
Analyses were conducted using SAS software (version 9.4) and Stata (version 16.1). Hazard ratios whose confidence intervals did not overlap 1.0 were considered as significant.
Patient and public involvement
No patients were involved in setting the research question, nor in the design, conduct, or interpretation of the study. The study is based on anonymised nationwide register data and there is no planned dissemination of results directly to study participants. Active elite football players were not involved in the study design and planning because it was not deemed crucial for conducting the study and because of resource (time and funding) constraints.
Results
Study population
The analyses included 6007 football players and 56 168 men from the general population. The median number of games played in the top tier of competition in Sweden among football players was 23 (interquartile range 6-76) (table 1). Football players had higher income than men from the general population, as well as higher scores for stress resilience, muscle strength, and cardiorespiratory capacity at military conscription (supplementary table 5).
Baseline characteristics of study groups
Primary outcome
During a mean follow-up time of 27.2 years, 257 (4.3%) football players and 3528 (6.3%) men from the general population experienced alcohol related disorders. The risk of alcohol related disorders was significantly lower among football players than among men from the general population (hazard ratio 0.71, 95% confidence interval 0.62 to 0.81; table 2).
Alcohol related disorders and disorders related to misuse of other drugs, among study groups
Additional analyses
The number of primary outcome events by year of first playing season in the Swedish top tier of competition among football players (and matched men from the general population) are shown in supplementary table 6. The hazard ratio and 95% confidence interval indicated no significant difference in risk of alcohol related disorders compared with men from the general population among football players who played their first season in the top tier before the 1960s, with the protective association emerging for those who played their first season in the early 1960s and later (fig 1).

Hazard ratios (95% confidence intervals) for alcohol related disorders among elite football players versus matched men from the general population, by the year of football players’ first season in the Swedish top tier of competition
{kind=link}
Analyses with the earliest cohort entry set to 2002 included 4159 football players and 33 361 men from the general population (supplementary table 7). Football players had a lower risk of alcohol related disorders than men from the general population (hazard ratio 0.66, 95% confidence interval 0.55 to 0.79). The hazard ratio was lowest at around age 35 years, and then increased with age; at around age 75 years, football players had higher risk than men from the general population (fig 2).
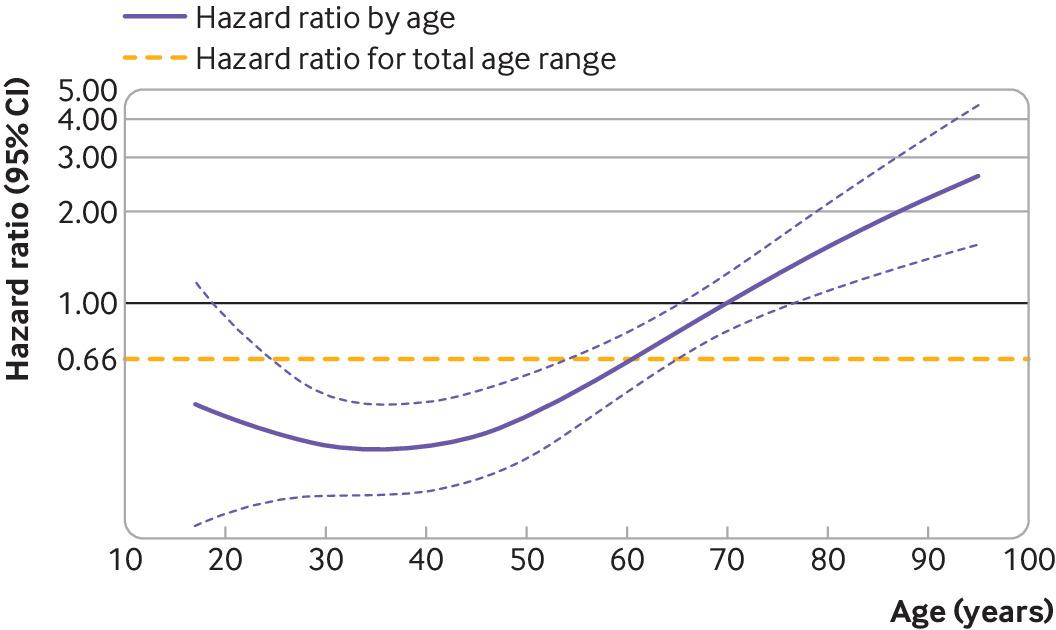
Hazard ratios (95% confidence intervals) for alcohol related disorders among elite football players versus men from the general population, by age
{kind=link}
In analyses restricted to football players, we saw no significant association between alcohol related disorders and goals scored per 10 games (supplementary fig 2), number of games (supplementary fig 3), or seasons played in the top tier (supplementary fig 4), although the hazard ratios tended to decrease with higher levels of these variables. The hazard ratio for outfield players versus goalkeepers was 1.12 (95% confidence interval 0.70 to 1.79).
Sensitivity analysis and exploratory analyses
Exclusion of participants aged ≥50 years at cohort entry yielded a similar hazard ratio to that of the primary analysis (table 3). Compared with analyses including all men from the general population with available data on income, the exclusion of men from the general population with zero registered income at cohort entry (hazard ratio 0.37 (95% confidence interval 0.24 to 0.57) v 0.41 (0.26 to 0.63)) and at age 40-44 years (0.45 (0.35 to 0.57) v 0.52 (0.41 to 0.66)) attenuated the association only slightly (table 3).
Sensitivity analysis and exploratory analyses
Of 2116 football players born between 1951 and 1987, 1889 (89%) had a registered result for at least one of the investigated tests, of whom 1673 (89%) had registered results from all investigated tests. We excluded four football players whose matched men from the general population did not have data for the investigated tests. Of 20 217 men from the general population born between 1951 and 1987, 17 605 (87%) had a registered result for at least one investigated test, of whom 15 745 (89%) had registered results from all investigated tests. We excluded 2199 men from the general population whose matched football players had no data from the investigated tests. Compared with analyses including individuals born in 1951-87 (hazard ratio 0.34, 95% confidence interval 0.26 to 0.46), the exclusion of individuals born in 1951-87 who did not have test results from military conscription (0.37, 0.27 to 0.52) did not materially affect the findings. Adjusting for cognitive ability and stress resilience attenuated the association (0.57, 0.41 to 0.79) while further adjustment for body mass index, muscle strength and cardiorespiratory exercise capacity had little impact on the result (0.58, 0.41 to 0.81; table 3).
Secondary outcome
The study population for the secondary outcome analysis included 4369 football players and 39 472 men from the general population (supplementary table 8). Football players had a significantly lower risk of disorders related to the misuse of other drugs than men from the general population (hazard ratio 0.22, 95% confidence interval 0.15 to 0.34; table 2).
Discussion
Main findings
This nationwide cohort study found that male football players in the Swedish top tier of competition had about 30% lower risk of alcohol related disorders than men from the general population who were matched on age and region of residence. Elite football players also had a lower risk of disorders related to the misuse of other drugs than men from the general population.
Interpretation and comparison with previous studies
Although alcohol and drug related disorders among active and retired elite athletes have been subject to much attention and research interest,13142829 large scale cohort studies assessing such outcomes are scarce. In accordance with our findings, one previous study from Scotland assessing a broad range of mental health related outcomes found that the risk of diagnoses related to alcohol use was lower among men who were former professional football players than among men from the general population (hazard ratio 0.62, 95% confidence interval 0.51 to 0.76).30 Taken together, the current evidence indicates that elite football players have a lower risk of alcohol related disorders during and after their career than men from the general population.
Potential mechanisms for the protective association observed in our study include that an elite football career might not be compatible with high alcohol consumption. In fact, many of the famous footballers who struggled with alcohol addiction had their careers severely impaired by their drinking habits.48 Although not significant, the hazard ratio for alcohol related disorders in our analyses tended to decrease with an increasing number of games and seasons played in the Swedish top tier of competition. Lower alcohol intake during adolescence and young adulthood could lead to reduced alcohol intake throughout the life course.3132 It is also likely that football players are more physically active than the general population. Physical exercise is hypothesised to reduce alcohol consumption and has been suggested as a treatment for alcohol related disorders,33 although some studies show an association between higher physical activity levels and risk of certain alcohol related disorders.3435 We also found that the elite football players had higher income than men from the general population, which could potentially protect against misuse of alcohol and other drugs.36
The lower risk of alcohol related disorders was observed among elite football players who played their first season in the Swedish top tier of competition in the 1960s and later, while football players from earlier eras had a similar risk as men from the general population. Professional football (as opposed to amateur football) was not allowed in Sweden until the late 1960s. In the first half of the 20th century, elite football players in Sweden received compensation from their clubs partly in the form of dinners and banquets with abundant alcohol consumption, and the commotion on trains caused by drunk footballers returning home from away games was repeatedly subject to public outcry.18 The role of alcohol consumption in Swedish football during this era might be indicated by a Liverpool FC player’s account of the game against AIK Stockholm during his team’s visit to Sweden in 1914: “I may say the spectators were disappointed at Liverpool’s play in the first half. As an excuse I might mention the fact that our boys had been entertained by the Swedish Football Association to a banquet the previous night, and that Swedish punsch, ‘the national beverage,’ has a bad after-effect!”37 After the second world war, some Swedish teams aimed to curb alcohol consumption among their players by introducing an increased daily allowance for those who abstained from the dinner drink. As elite football became a full time occupation for many players and competition increased among players, reports of alcohol consumption among elite football players decreased.18
The lower risk of a registered alcohol related disorder was more pronounced at ages when the football players are typically active in their professional careers. By contrast with the hypothesis that the risk of alcohol related disorders might increase shortly after the retirement from elite football, the risk for football players versus men from the general population was lower also after the typical age of retirement for football players. However, the association gradually weakened with increasing age and from around age 75 years, football players had a higher risk than men from the general population. This pattern might be due to a depletion of men from the general population who are susceptible to alcohol related disorders38 and the lack of a protective association for football players in older birth cohorts, as indicated in the analyses by calendar year of the first season played in the top tier of competition.
Limitations of the study
Our study had limitations. Firstly, outcome events were captured using diagnoses registered in death certificates, during hospital and outpatient care visits, and filled prescriptions for drugs used to treat alcohol addiction. Depending on individuals’ health seeking behaviour and clinical manifestations of alcohol addiction, substantial amounts of time could have passed between the start of alcohol addiction and the registration of the outcome event in the registers. Moreover, individuals could have had alcohol related disorders without receiving a diagnosis, although the likelihood of such an outcome misclassification is unlikely to differ between football players and men from the general population.
Secondly, owing to data availability, we could not use all ICD codes describing conditions related to alcohol use.3940 Thirdly, we did not have access to data on family histories of alcohol related disorder, which might have differed between football players and men from the general population. Finally, our study included male elite football players and the generalisability of our findings to female elite players and to male and female amateur and youth players (who constitute most football players worldwide) is uncertain. Alcohol is ingrained in the fan culture surrounding football,4 which amateur players, given their interest in the sport, might be part of. Moreover, many studies have shown that participation in some sports (eg, football, ice hockey, and basketball) is associated with higher alcohol intake.41
What is already known on this topic
Alcohol consumption has been deeply ingrained in football culture for both players and fans, and several well known players have experienced alcohol addiction during and after their active playing careers
What this study adds
In this nationwide cohort study, male football players who played in the Swedish top tier of competition in 1924-2019 had a lower risk of diagnosis of alcohol related disorders than men from the general population (hazard ratio 0.71, 95% confidence interval 0.62 to 0.81)
This reduced risk was observed among football players who played their first season in the top tier from the early 1960s onwards; the protective association was most pronounced at around age 35 years and weakened with increasing age
Ethics statements
Ethical approval
The study was approved by the Swedish Ethical Review Authority (2021-04248). Informed consent was not required.
Data availability statement
No additional data available. The data analysed in this study were based on Swedish nationwide registers. Individual level data in the registers can only be accessed through secure servers and only export of aggregated data, as presented in research articles, is allowed as per Swedish law. Permission to access data can be made only after fulfilling specific requirements to safeguard the anonymity of the study participants. For these reasons, data cannot be made generally available.
Footnotes
Contributors: MK, BP, and PU conceived and designed the study. All authors contributed to the acquisition, analysis, and interpretation of data. MK and PU did the statistical analysis. PU drafted the report. All authors critically revised the report for important intellectual content. PU and BP obtained funding for the study. All authors approved the final manuscript. PU and MK are guarantors for this study. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding: The study was funded via unrestricted research grant support from the Strategic Research Area Epidemiology programme at Karolinska Institutet, Swedish Research Council for Sport Science, Folksam Research Foundation, Hedberg Foundation, Neurofonden, and Åhlen Foundation. BP was supported by a consolidator investigator grant from Karolinska Institutet. The funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: support from the funding bodies listed above for the submitted work; MF is the chairman of the Swedish Football Association’s medical committee and member of the medical committees of UEFA and FIFA, the European and world football bodies, respectively; the other authors declare no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influence the submitted work.
The lead authors (MK and PU) affirm that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Dissemination to participants and related patient and public communities: The results of this research will be disseminated via the websites of the authors’ institutes. As the study is based on pseudonymised register data, there is no planned dissemination of results directly to study participants. We plan to post information about the study on our personal Karolinska Institutet websites. As we aim to publish additional studies on health outcomes among football players, we plan to write a blog post for The BMJ to summarise the current evidence.
Provenance and peer review: Not commissioned; externally peer reviewed.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.