Diagnosis and management of covid-19 in pregnancy
BMJ 2022; 377 doi: https://doi.org/10.1136/bmj-2021-069739 (Published 26 April 2022) Cite this as: BMJ 2022;377:e069739
- Melanie Nana, obstetric medicine fellow1,
- Kenneth Hodson, consultant in obstetrics and maternal medicine2,
- Nuala Lucas, consultant anaesthetist3,
- Luigi Camporota, consultant in intensive care medicine1,
- Marian Knight, professor of maternal and child population health4,
- Cathy Nelson-Piercy, professor of obstetric medicine1
- 1Guys and St Thomas’ NHS Foundation Trust, London, UK
- 2Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle upon Tyne, UK
- 3Northwick Park Hospital, London, UK
- 4National Perinatal Epidemiology Unit, Nuffield Department of Population Health, University of Oxford, UK
- Correspondence to: M Knight Marian.knight{at}npeu.ox.ac.uk
- Series explanation: State of the Art Reviews are commissioned on the basis of their relevance to academics and specialists in the US and internationally. For this reason they are written predominantly by US authors
Abstract
Pregnant women with covid-19 are at greater risk of severe disease than their non-pregnant peers, and yet they are frequently denied investigations or treatments because of unfounded concerns about risk to the fetus. The basic principles of diagnosing and managing covid-19 are the same as for non-pregnant patients, and a multidisciplinary, expert team approach is essential to ensure optimal care. During pregnancy, treatment with corticosteroids should be modified to use non-fluorinated glucocorticoids. Il-6 inhibitors and monoclonal antibodies, together with specific antiviral therapies, may also be considered. Prophylaxis against venous thromboembolism is important. Women may require respiratory support with oxygen, non-invasive ventilation, ventilation in a prone position (either awake or during invasive ventilation), intubation and ventilation, and extracorporeal membrane oxygenation (ECMO). Pregnancy is not a contraindication for any of these supportive therapies, and the criteria for providing them are the same as in the general population. Decisions regarding timing, place, and mode of delivery should be taken with a multidisciplinary team including obstetricians, physicians, anesthetists, and intensivists experienced in the care of covid-19 in pregnancy. Ideally these decisions should take place in consultation with centers that have experience and expertise in all these specialties.
Introduction
Pregnant women appear no more or less likely to contract SARS-CoV-2 infection than the background population. However, as with other viral illnesses, including influenza and varicella, the risk of developing severe disease is increased in pregnant patients compared with their non-pregnant counterparts, particularly if they contract the infection in the third trimester of pregnancy.12 SARS-CoV-2 infection in pregnancy is associated with a higher risk of morbidity and mortality for both mother and fetus compared with pregnant women without infection.134 The chance of developing severe disease that requires respiratory support, admission to an intensive care unit, and invasive ventilation are increased compared with those who are infected and not pregnant.5 These increased risks in pregnancy have become more marked with successive variants of SARS-CoV-2 and are highest for the delta variant24 (although data are still emerging on the impact of the omicron variant). Vaccination rates remain low among many populations of pregnant women, and ensuring that pregnant women with covid-19 receive timely and evidence based care will continue to be important for the foreseeable future.
Diagnosis and management of covid-19 in pregnancy is, for the most part, the same as in non-pregnant patients. However, important investigations such as chest radiographs and lung computed tomography (CT) are frequently withheld on account of pregnancy status, because of unsubstantiated concerns regarding fetal safety. Similarly, despite improvements allowing pregnant women to be recruited into important trials exploring effective therapies for covid-19, and a sound evidence base for treatments such as corticosteroids and IL-6 inhibitors,67 pregnant women are not being offered these therapies as is routine in non-pregnant patients.2 Unfounded concerns for the fetus contribute to therapeutic inertia, such that potentially lifesaving therapies are denied to pregnant women. Special consideration is required when managing pregnant women who are severely ill with covid-19 and have developed covid-19 acute respiratory distress syndrome. This includes women who require respiratory support with oxygen, non-invasive ventilation, ventilation in a prone position (either awake or during invasive ventilation), intubation and ventilation, and extracorporeal membrane oxygenation (ECMO). Pregnancy is not a contraindication for any of these supportive therapies, and criteria for delivering these treatments and therapeutic targets are the same as for the general population and should be respected to avoid unnecessary morbidity and mortality.
This review is an in depth reference guide for all clinicians and allied healthcare professionals who treat pregnant women with covid-19. It may be particularly useful for those who work in emergency medicine, general medicine, anesthetics, and intensive care, who may be less familiar with the physiological changes associated with pregnancy and less confident in their knowledge of therapeutic options available. Treatment must not be withheld in pregnancy for fear of causing harm to the fetus, since this puts both mother and baby at risk from significant morbidity and mortality. This comprehensive review of evidence on treatment of covid-19 in pregnancy includes therapies currently in development or testing and not yet in routine use. As treatments for covid-19 rapidly evolve, clinicians are advised to refer additionally to the most up-to-date guidance from national institutions (such as the Society for Maternal Fetal Medicine, or the Royal College of Obstetricians and Gynaecologists in the UK) when managing covid-19 in pregnant women.8
Sources and selection criteria
We identified articles and other relevant information through a manual search of electronic databases PubMed and the Cochrane Library for English language articles, published from 1 January 2020 to 21 December 2021, further updated on 17 January 2022. We undertook a broad search using Mesh terms “COVID-19” and “pregnancy” combined with the terms “therapy”, “etiology”, and “prognosis”. For specific therapeutic options where we could identify no high quality pregnancy specific studies, we removed the term “pregnancy” and restricted the search on the basis of specific medication classes—eg, “corticosteroid”, “monoclonal antibody”, and “anti-viral”. Searches were augmented by information from monographs produced by the UK Teratology Information Service following systematic literature review and analysis of teratology database data available to health professionals in the Toxbase database. We supplemented epidemiological data from published studies with published data from the organizations responsible for national surveillance of covid-19 in pregnancy and pregnancy outcomes (eg, US Centers for Disease Control and Prevention, and UK Confidential Enquiry into Maternal Deaths). In view of the continually emerging information, we also obtained in-press peer reviewed articles from authors, where the data had been publicly presented and were therefore known to inform the review. We limited the literature used to systematic reviews, large randomized controlled trials (RCTs), high quality population based observational studies which we considered at low risk of bias, and guidelines. Where no other literature was identified we report case series.
Epidemiology, clinical features, and risk factors for severe covid-19
The reported incidence of covid-19 infection in the obstetric population varies by geographical region, testing period during the pandemic, and method of testing. Figures from the US as of 21 March 2022 indicate that 193 980 pregnant women have had covid-19, and 270 of these (1.4 per 1000 with infection) have died.9 Sixteen per cent of pregnant women with covid-19 (31 211 women) have been admitted to hospital.10 A World Health Organization living systematic review reported an overall rate of SARS-CoV-2 infection of 10% (95% confidence interval, CI 7% to 12%) in pregnant and recently pregnant women attending or admitted to hospital for any reason. However, of the women tested under universal screening policies, an incidence of 7% (95% CI 5% to 8%) was reported, and this increased to 28% (95% CI 15% to 43%) for women tested based on symptoms.1
Minority ethnicity has consistently been identified as being associated with a higher risk of being admitted to hospital with covid-19 in pregnancy. In a retrospective cohort study from the US, Hispanic and non-Hispanic black pregnant women accounted for nearly half of all cases of covid-19, despite constituting approximately one third of the study population.11 In a prospective study from the UK in the initial pandemic wave of infection, pregnant women from black or other ethnic minority groups accounted for 56% of all admissions12; this decreased in later waves.13
Around 9% of pregnant or recently pregnant women with covid-19 develop severe infection, and 4% require admission to intensive care (odds ratio, OR, compared with non-pregnant women of reproductive age with covid-19, 2.13, 95% CI 1.53 to 2.95) and 2% go on to receive invasive ventilation (OR 2.59, 95% CI 2.28 to 2.94).1 Additionally, pregnant women with covid-19 are at an increased risk of maternal death (OR 2.85, 95% CI 1.08 to 7.52).2
The World Health Organization living systematic review shows that pregnant women are less likely to develop symptoms than their non-pregnant counterparts,1 although the number of included women in that comparison was small. Symptoms, for those who develop them, are usually mild, and most frequently include cough (41%), fever (40%), dyspnea (21%), and myalgia (19%). However, the evidence in this systematic review suggests a different pattern of symptoms between pregnant and non-pregnant women. Pregnant women are less likely to exhibit fever (OR 0.49, 95% CI 0.38 to 0.63), breathlessness (OR 0.76, 95% CI 0.67 to 0.85), or myalgia (OR 0.53, 95% CI 0.36 to 0.78) than non-pregnant women.1 The differing symptom pattern needs to be recognized in clinical protocols used for diagnosis or to triage referrals in the community; a rapid report on maternal deaths related to covid-19 from the UK Confidential Enquiries into Maternal Deaths highlighted an instance of a pregnant woman who died at home from covid pneumonitis after a misdiagnosis of an upper respiratory tract infection following a protocol guided telephone consultation.14 The report indicates that it was unclear whether the protocol had taken into account the different pattern of symptom presentation in pregnant women. The reasons for differing symptoms are not clear, but may reflect an overlap of the pathophysiology of covid-19 with the physiology of pregnancy, a phenomenon that has been noted with other types of disease in pregnancy.1516
Severe disease during pregnancy is typically a phenomenon of the late second or third trimesters. A UK national cohort study of women admitted to hospital with symptomatic covid-19 in pregnancy showed that most were in the second half of pregnancy and more than three quarters were in the third trimester.2 Linked data from Scotland show that, while infections occur evenly throughout pregnancy, 7% of first trimester infections were associated with hospital admission, compared with 11% in the second trimester, and 34% in the third trimester.17 Risk factors for severe disease are similar to those in non-pregnant individuals and include age over 35, obesity, minority ethnicity, and comorbidities including pre-existing lung conditions, hypertension, and diabetes.3101318 The increased risk associated with ethnic minority backgrounds has been shown in women who are pregnant and those who are not, with health inequalities and socioeconomic factors proposed as contributing factors. Note, however, that ethnic disparities in hospital admission rates with covid-19 in pregnancy are not consistently reflected in higher risks of severe infection.113 Severe infection is most consistently associated with older maternal age, raised body mass index, and chronic hypertension.11319
The patterns of disease in pregnancy appear to have changed over the periods in which different SARS-CoV-2 variants were predominant. Compared with periods where wild type SARS-CoV-2 was prevalent, a US study reported that pregnant women were 11% more likely to have moderate to severe infection if infected during an alpha prevalent period, and 9% more likely during a delta compared with an alpha period. Those admitted in the alpha period were more likely than those admitted during a wild type period to require respiratory support (27.2% versus 20.3%), have pneumonia (27.5% v 19.1%), and be admitted to intensive care (11.3% v 7.7%). Women admitted during the delta period had further increased risk of pneumonia when compared with the alpha period (36.8% v 27.5%). As the delta variant predominated, both the case volume and proportion of severely or critically ill women increased (fig 1).

Proportion of pregnant patients with severe to critical illness increased as the delta variant of SARS-CoV-2 predominated (shown in blue). Graph adapted from20
{kind=link}
Similar changes in severity have been reported in the UK, Italy, and the Netherlands with changing variant type.22122 In the period during which the delta variant predominated in the UK, 16% of symptomatic pregnant women admitted to hospital were admitted to an intensive care unit,2 and one in five of all patients receiving ECMO were women who were pregnant or post partum.23 The risk of severe disease among unvaccinated women during the omicron period was comparable with that observed during the wild type period.24
Clinical investigation and diagnosis
As with all medical problems in pregnancy, priority should be given to confirming a diagnosis and stabilizing the woman’s condition with standard investigations and therapies and not withholding these inappropriately owing to fetal concerns. Clinicians must recognize that reference ranges for relevant investigations are different in pregnancy (table 1). Reviews of maternal deaths from covid-19 have highlighted several instances where the severity of women’s illness has not been recognized owing to a lack of understanding of relevant reference ranges in pregnancy, in particular that respiratory rate and oxygen saturations do not change in pregnancy.2627
Reference ranges of relevant investigations in non-pregnant and pregnant populations25
Pregnant women with suspected covid-19 should not be denied imaging in the form of chest radiography, ventilation/perfusion (V/Q) scan, or computed tomography pulmonary angiography (CTPA) where indicated. Fetal radiation and maternal breast radiation doses are described in table 2. Women can be reassured that a transatlantic flight is associated with radiation exposure one to six times that of a chest radiograph.29 Chest radiography and CTPA changes in pregnant women with covid-19 are similar to those in non-pregnant individuals, usually showing bilateral consolidation, and sometimes accompanied by pneumothoraxes or pneumomediastinum (figs 2, 3).
Safety of commonly used radiological imaging28

Bilateral airspace opacities in a pregnant patient with covid-19 pneumonitis
{kind=link}
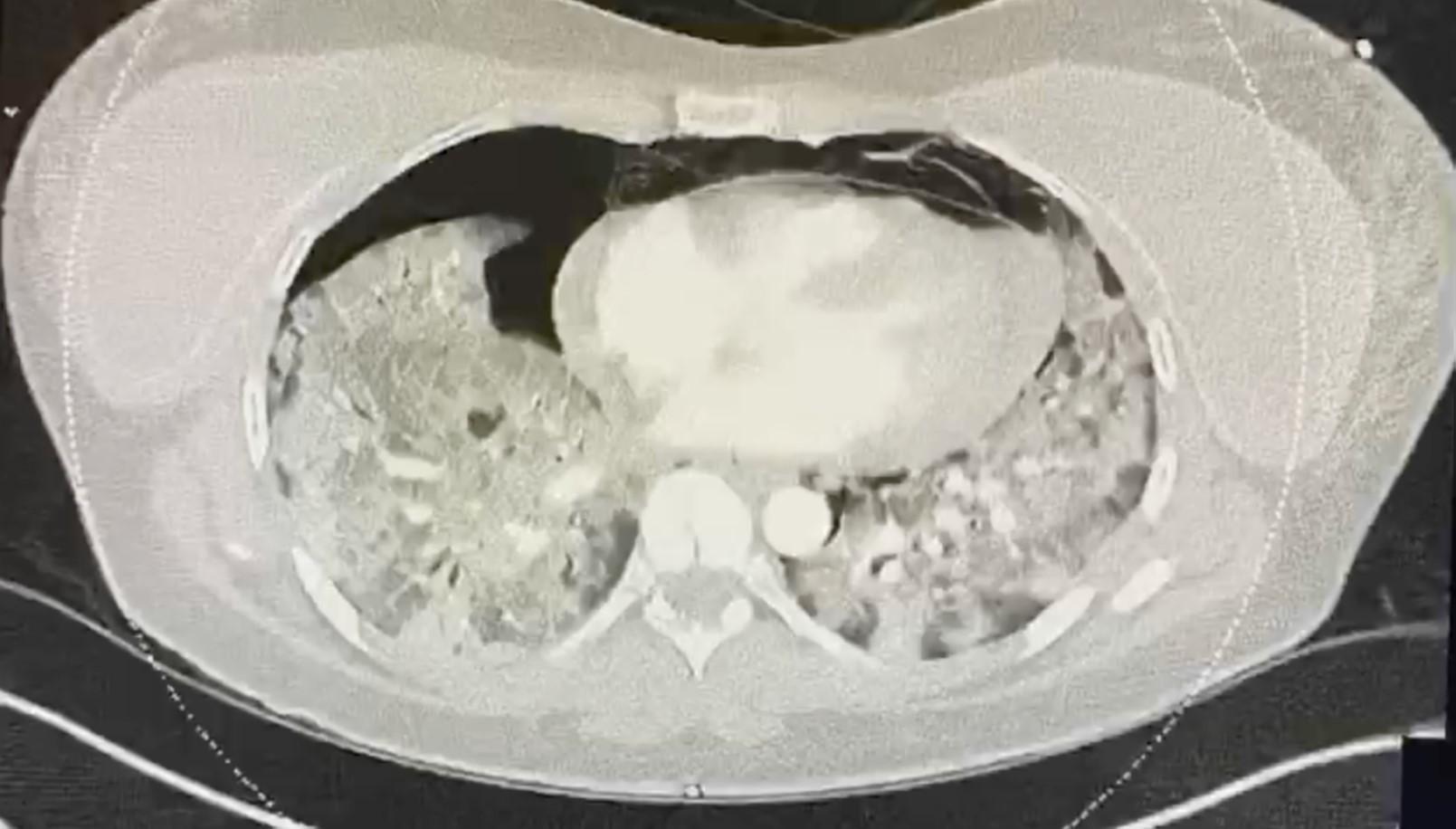
CTPA showing widespread consolidation within both lungs with surrounding ground glass opacification, moderately sized right sided pneumothorax, small volume left sided pneumothorax in a patient with covid-19
{kind=link}
Management
Rapid advances have been made in the development of evidence based therapies for managing covid-19, most of which are acceptable to use in pregnancy when considered on a benefit-to-risk assessment. However, data have shown that only around a quarter of pregnant women who would benefit from such therapies receive them, even when admitted to an intensive care unit.230 Management in pregnancy must reflect, as closely as possible, management outside pregnancy. When clinicians are uncertain about the use of treatments in pregnancy, they should seek urgent advice—eg, via obstetric physicians or expert obstetricians, to minimize maternal morbidity and mortality. The Royal College of Obstetricians and Gynaecologists in the UK has maintained a frequently updated guideline on managing covid-19 in pregnancy.8 The American College of Obstetricians and Gynecologists offers practice advisory guidance and an algorithm on “outpatient assessment and management for pregnant women with suspected or confirmed novel coronavirus (covid-19).” 31
An approach to clinical management of covid-19 in women who are pregnant or up to six weeks post partum is outlined in figure 4. Input from a multidisciplinary team is essential, with prompt escalation involving senior decision makers if a patient’s condition deteriorates.

Approach to clinical management of covid-19 in women who are pregnant or up to six weeks post partum. This figure is based on guidance produced by the Royal College of Obstetricians and Gynaecologists (RCOG)8 and incorporates the RCOG VTE Prevention Green Top Guideline32 and Interim Clinical Commissioning Policy: Antivirals or neutralizing monoclonal antibodies in the treatment of COVID-19 in hospitalised patients (Version 5).33ACOG=American College of Obstetricians and Gynecologists; CPAP=continuous positive airway pressure; ECMO=extracorporeal membrane oxygenation; LMWH=low molecular weight heparin; RR=respiratory rate; VTE= venous thromboembolism
{kind=link}
Pharmacological management
Corticosteroids
A Cochrane review of the use of systemic corticosteroids for patients admitted to hospital with covid-19 included nine RCTs and concluded that moderate certainty evidence showed that administration reduced all cause mortality (risk ratio, RR, 0.89, 95% CI 0.80 to 1.00; 7930 participants).34 The largest of the included trials, RECOVERY, showed that low dose dexamethasone reduced mortality by one fifth in patients with covid-19 receiving oxygen, and by one third in those requiring mechanical ventilation.6 However, dexamethasone readily crosses the placenta, and repeated doses in pregnancy have been associated with neurocognitive and neurosensory disorders in childhood.35 Pregnant women who were recruited into the RECOVERY trial were therefore given either oral prednisolone or intravenous hydrocortisone, both of which (in contrast to dexamethasone) are non-fluorinated glucocorticoids which are therefore extensively metabolized by placental enzymes, crossing the placenta in small amounts only3637 (fig 5). A similar pattern of conversion is seen with methylprednisolone.38 Evidence does not suggest any harm from non-fluorinated corticosteroid use in pregnancy.39 The Cochrane review included seven small trials that investigated either methylprednisolone or hydrocortisone; the estimated relative risk reduction in mortality was of similar magnitude to that seen in the trials of dexamethasone, although did not reach statistical significance.34 Nevertheless, this provides supportive evidence for the benefit of other steroids for pregnant women with covid-19 as an alternative to dexamethasone. The most appropriate choices of corticosteroids for treatment of maternal covid-19 in pregnancy therefore include oral prednisolone 40 mg once daily or intravenous hydrocortisone 80 mg twice daily. Oral methylprednisolone 32 mg once daily or an intravenous dose of 1 mg/kg twice daily may also be considered, particularly if the patient is in an intensive care unit (ICU) setting.8 Recommendations on corticosteroid regimens vary by geographical location, however, because RCT evidence explicitly in the pregnant population with covid-19 is lacking. These are recommended corticosteroid regimens, but decisions should be made on an individual basis.

Corticosteroids prednisolone, hydrocortisone, and methylprednisolone are non-fluorinated glucocorticoids and thus converted by 11β-hydroxysteroid dehydrogenase 2 (11β-HSD2) into inactive metabolites in the syncytiotrophoblasts of the placental villi. Only small amounts of the active metabolite are able to pass the placenta into the fetal circulation, making these the corticosteroids of choice for treatment of maternal covid-19 disease. Dexamethasone and betamethasone, fluorinated glucocorticoids, are less extensively metabolized by 11β-HSD2 and thus cross the placenta more readily, making them the appropriate corticosteroids of choice for fetal lung maturation. GCs=glucocorticoids
{kind=link}
The use of dexamethasone and betamethasone (both fluorinated glucocorticoids) should be reserved for fetal lung maturity only.40 In such cases, on the day of administration, the corticosteroids used for maternal disease should be omitted. Outside the ICU setting, corticosteroid therapy should be given for 10 days or up until hospital discharge, whichever is sooner.8 For patients admitted to ICU, decisions about steroid duration should be made on an individualized basis. Clinicians should consider prescribing a proton pump inhibitor to women given steroids to prevent gastric irritation; these can be given safely in pregnancy. Corticosteroids and concurrent illness affect glucose metabolism and may cause hyperglycemia, leading to gestational diabetes. Capillary blood glucose levels should be monitored and sustained high glucose levels treated accordingly.41
Prospective controlled studies suggest that non-fluorinated corticosteroids are not harmful in pregnancy.42 The risks of fetal malformation, pregnancy loss, or intrauterine death are not increased in women using corticosteroids during pregnancy.39 Studies showing increased rates of fetal growth restriction, preterm premature rupture of the membranes, preterm birth, and pre-eclampsia are likely to be confounded by underlying health conditions for which corticosteroids have been prescribed.43
Interleukin-6 receptor antagonists
A systematic review of the use of interlukin-6 receptor (anti-IL6) antagonists for patients admitted to hospital with covid-19 concluded that evidence of high certainty suggests tocilizumab reduces all cause mortality at day 28 compared with standard care alone or placebo (RR 0.89, 95% CI 0.82 to 0.97; 8 RCTs, 6363 participants).44 Evidence was insufficient, however, to be certain about sarilumab, although the reviewers noted that the magnitude of the estimate of relative mortality reduction was similar to that observed in tocilizumab trials.
Tocilizumab was shown in the RECOVERY trial to improve survival in patients admitted to hospital with covid-19 who had hypoxia (oxygen saturation <92% on air or requiring oxygen therapy) and evidence of systemic inflammation (C reactive protein ≥75 mg/L). The benefits were seen regardless of the degree of respiratory support and were in addition to the benefits of corticosteroids.6
Limited data are available to support the safety of tocilizumab in pregnancy. Data consist of uncontrolled case reports or series, which together describe approximately 600 exposed pregnancies.45 Although adverse outcomes in pregnancy have been described (including cases of congenital anomaly, pregnancy loss, and preterm deliveries), the crude rates of these events do not generally appear notably increased above the background rate. Published reports of tocilizumab use outside covid-19 largely include exposure in the first trimester, when transplacental transfer is expected to be negligible; in these patients congenital malformation rates are comparable with background rates. In the limited data for the use of tocilizumab in pregnant patients with covid-19, administration is most frequently in the third trimester and in all cases reported to date, the pregnancies have resulted in live births.46 Tocilizumab is excreted in very low levels in breast milk and is not considered a contraindication to breastfeeding.47
Sarilumab, a similarly acting IL-6 receptor monoclonal antagonist, can be substituted if tocilizumab is unavailable.48 Use of IL-6 receptor antagonists is reserved for those who have moderate to severe covid-19; therefore, the benefits of giving treatment are likely to outweigh any theoretical risk to the fetus. Currently, risks to the fetus are unknown, but not thought to be significant given the mechanism of action of the medication, animal data, and limited but reassuring data on pregnancy safety when using tocilizumab. No evidence suggests that sarilumab is harmful.
Recommendations are that neonates exposed in utero to biologic drugs that modify immunity (eg, TNF-α inhibitors and IL-6 receptor blockers) have live vaccination no sooner than six months following birth. This includes vaccinations for rotavirus and Bacillus Calmette-Guérin (BCG) vaccinations. The recommendation followed a reported fatal case of disseminated tuberculosis following BCG vaccination in a neonate born to a woman who was taking infliximab during pregnancy.49 Monoclonal antibodies specifically targeting viral proteins (such as the neutralizing monoclonal antibodies sotrovimab and ronapreve) do not modify human immunity and therefore live vaccines can be given to these neonates.
Women given tocilizumab or sarilumab should be informed that they may be more susceptible to infection for up to six months following treatment.50 If they feel unwell they should seek medical attention early and make their healthcare provider aware of the increased risk of infection.
Neutralizing monoclonal antibodies
Several SARS-CoV-2 neutralizing monoclonal antibodies have been developed or are in development. A Cochrane review published in September 2021 identified six completed and 31 ongoing studies. Small studies of patients not admitted to hospital evaluated bamlanivimab, sotrovimab, regdanvimab, and combinations of bamlanivimab/etesevimab, and casirivimab/imdevimab. Certainty of the evidence of impact on all outcomes examined was low because of too few events. Bamlanivimab and casirivimab/imdevimab were evaluated in patients admitted to hospital, with robust evidence available only for casirivimab/imdevimab. These monoclonal antibodies, directed toward the SARS-CoV-2 spike protein, were shown in the RECOVERY trial to be beneficial,51 in particular to patients who have not developed innate immunity to covid-19 (ie, do not have natural SARS-CoV-2 antibodies), with a reduction in 28 day mortality (RR 0.80; 95% CI 0.70 to 0.91; 3153 seronegative patients).51 The trial included pregnant participants.
Data on safety for monoclonal antibodies in pregnancy are lacking; however, since the monoclonal antibodies are uniquely directed toward viral proteins, interference with fetal development is unlikely. Furthermore, other types of monoclonal antibody are commonly given in pregnancy (examples include anti D) with no adverse effects on the developing fetus. Reporting of the pregnancy to a teratology information service or national registry is encouraged so that safety data can be acquired.
Casirivimab/imdevimab should therefore be considered in women who are admitted to hospital with symptomatic covid-19 and who do not have SARS-CoV-2 antibodies. The use of casirivimab/imdevimab to treat covid-19 in seronegative pregnant women in hospital, however, must take account of the prevalent SARS-CoV-2 variant, as recent studies have shown that both these and some other monoclonal antibodies do not retain activity against the omicron variant.52535455
Sotrovimab, which has been shown to reduce progression to hospital admission or death in patients with mild to moderate covid-19,56 has retained activity against the omicron variant,54 and may therefore be considered for pregnant patients at risk of progression to severe disease. Its efficacy to improve outcomes among patients admitted to hospital, however, has not yet been established, and further trials are in progress.57 No data are available for the use of sotrovimab in pregnancy. However, in a cross reactive binding assay, no off-target binding was detected using a protein array enriched for human embryo-fetal proteins. Being a human immunoglobulin G, sotrovimab has the potential for placental transfer, but where the expected benefit to the mother justifies this theoretical risk, it may be used in pregnancy.58
Antivirals
Numerous antiviral medications have been proposed and tried for the treatment of covid-19. Lopinavir/ritonavir and interferon β have been shown not to be of benefit, and their routine use is not advised. In November 2020 the World Health Organization issued a conditional recommendation against the use of remdesivir for the management of acute covid-19 infection because of lack of evidence of efficacy. Limited data exist for pregnancy safety, and remdesivir is not routinely recommended in pregnancy.
Other, new antiviral agents that have been developed since the beginning of the pandemic are showing promising results. Molnupiravir is an antiviral prodrug that inhibits viral replication through the active metabolite being incorporated into the viral RNA, resulting in an accumulation of errors in the viral genome. In the UK, it is licensed as a five day course for the treatment of mild to moderate covid-19 in adults with a positive diagnostic test result for SARS-COV-2, who have at least one risk factor for developing severe illness. However, concerns have been expressed about the safety of molnupiravir in pregnancy. Preclinical data on animal reproductive toxicity are conflicting, with high maternal doses administered in rat models showing possible teratogenic effects, but no evidence of similar effects observed in rabbit models.59 No human data exist regarding the safety of molnupiravir in pregnancy. Given the mechanism of action and animal data, molnupiravir is not currently recommended for use in pregnancy. Reporting a pregnancy to a reproductive toxicology registry60 is encouraged if pregnant women are inadvertently given molnupiravir, so that safety data can be acquired.
Paxlovid (nirmatrelvir/ritonavir) is licensed for the treatment of covid-19 in adults who do not require supplemental oxygen, but who are at increased risk of developing severe illness.61 Nirmatrelvir works through inhibition of the coronavirus 3C-like (3CL) protease, thereby preventing viral replication. Co-administration with ritonavir (a protease inhibitor commonly used for treating HIV) is necessary to inhibit the CYP3A mediated metabolism of nirmatrelvir. Ritonavir does not have pharmacodynamic activity against SARS-CoV-2 3CL protease. Paxlovid has been shown to significantly reduce admission to hospital and mortality when given in the first three days from symptom onset in a selected, high risk, non-pregnant population. Whether this translates into benefit in pregnant women is the subject of ongoing studies (including RECOVERY). Although no pregnancy safety data exist relating to its use in human pregnancy, animal toxicology studies have not identified adverse effects on fetal morphology or embryo-fetal viability in rat or rabbit models with doses of nirmatrelvir up to 12 times the human equivalent dose. In the offspring of pregnant rabbits administered 24 times the equivalent human dose, lower fetal body weights were observed, but evidence of maternal toxicity was also described with an impact on maternal weight gain/food consumption, which may explain the fetal effects. Ritonavir has an established safety profile relating to its use in treating HIV in pregnancy, with no particular safety concerns.62 Paxlovid has the potential to interact with other medications, through liver enzyme CYP3A inhibition. Clinicians are advised to check the product characteristics documentation carefully for potential drug interactions when other medications are co-administered. At the time of writing, the role of paxlovid in treating pregnant women with covid-19 is yet to be fully established; however, despite the lack of human pregnancy safety data for paxlovid, in specific circumstances, where the benefits of use during pregnancy could outweigh the risks, its use might be acceptable. Such circumstances may include use in women at high risk of developing severe disease (owing to non-vaccination status or clinical vulnerabilities), or in women experiencing severe symptoms of covid-19 where other more established treatments have failed.
Preventing venous thromboembolism
Pregnant women and those in the postpartum period who have intercurrent illness are at increased risk of venous thromboembolism (VTE). Thus, all women presenting with covid-19 should be advised to stay hydrated, mobile, and should undergo risk assessment for VTE (fig 4). All pregnant women admitted to hospital with covid-19 should be given thromboprophylaxis, unless contraindicated, during their inpatient admission. Although a randomized controlled trial suggested a beneficial effect for therapeutic versus prophylactic heparin in non-critically ill patients with covid-19, no benefit was seen in critically ill patients, 6364 and no pregnant women were enrolled in the trial. Current UK practice does not recommend therapeutic doses of low molecular weight heparin (LMWH) in covid-19, except in those with suspected or proven VTE.
A discussion with the multidisciplinary team should take place for women in whom imminent delivery is anticipated, so that the dose of LMWH can be timed appropriately to allow for regional anesthesia, which ideally requires prophylactic dose LMWH to be withheld for 12 hours and therapeutic dose LMWH for 24 hours beforehand.
Maternal critical care
The threshold should be low for referring pregnant women with moderate or severe covid-19 to critical care support. Pregnant women are typically able to compensate for prolonged periods before their condition rapidly deteriorates. Vigilance should be paid to subtle changes in deterioration, with prompt escalation to senior clinicians (ideally an obstetric physician, obstetrician, or obstetric anesthetist and intensivist with expertise in the care of pregnant women with medical problems) for those showing signs of deterioration. Intensive care management of pregnant women largely mirrors that outside pregnancy. Clinicians should seek to establish breastfeeding preferences for women who may undergo sedation for invasive ventilatory support, so that in this circumstance breastfeeding can be supported until the patient is awake.
Respiratory support
Most of the basic respiratory support principles utilized in the non-pregnant population apply equally to pregnant women. The initial intervention for hypoxemic pregnant patients with covid-19 is the administration of oxygen therapy, usually with nasal cannula or a face mask. Supplemental oxygen should be titrated to achieve an oxygen saturation of 94-98%. Although some lower thresholds are recommended, no evidence supports this practice. Oxygen therapy can be escalated with various devices, dependent on local resources, including venturi masks, non-rebreather masks, high flow nasal cannula, and non-invasive positive airway pressure (eg, continuous positive airway pressure, CPAP, or non-invasive ventilation, NIV, which includes the setting of an inspiratory pressure support in addition to the CPAP level).65 Interaction between the increased cardiac output, which occurs later in pregnancy, and the alterations in ventilation/perfusion distribution characteristic of covid-19, make pregnant women more likely to develop more severe hypoxemia than non-pregnant patients with the same degree of lung involvement. This means that, given the same degree of lung consolidation, the higher cardiac output increases the functional pulmonary shunt, leading to worse hypoxemia, particularly in covid-19, where the pathophysiology of hypoxemia is initially and primarily due to an increased functional and anatomical (through neovascularization) shunting of affected lung regions.6667 In addition, the reduction in lung volumes owing to the pregnant uterus may increase lung strain for the same inspiratory volume and may increase the risk of lung injury (eg, pneumomediastinum) when the inspiratory effort is high and not controlled by non-invasive or invasive ventilation. Finally, although hypercapnia may be less common in this population given the hyperventilation and the fact that the high cardiac output will reduce the lung regions with high ventilation/perfusion ratio, note that, when developed, this indicates a worse severity of lung disease.
Intubation and ventilation should be undertaken with the same indications as for non-pregnant patients, however, appreciation of the physiological changes induced by covid-19 and pregnancy should guide the most appropriate timing. The RECOVERY-RS trial examined the effect of CPAP, high flow nasal oxygen, and conventional oxygen therapy on respiratory outcomes in patients with covid-19.6869 The authors found that, compared with conventional oxygen therapy, CPAP significantly reduced intensive care admission rates (54.1% v 61.5%, OR 0.74), the requirement for intubation (33.4% v 41.3%, OR 0.71), and 30 day mortality (16.7% v 19.2%, OR 0.84). For high flow nasal oxygen versus conventional oxygen therapy, no significant difference was seen in intensive care admission, time to intubation, duration of mechanical ventilation, critical care length of stay, or length of hospital stay. However, other studies have shown a significantly decreased need for mechanical ventilation support and time to clinical recovery using high flow nasal oxygen or NIV70 depending on settings and availability of interface. Therefore, escalation from low flow to high flow oxygen may be appropriate provided that the inspiratory effort and breathlessness are low. With higher FiO2 (eg, >0.6) and increased inspiratory effort, a trial of CPAP or NIV is supported by recent evidence. However, clinicians must stay vigilant and choose appropriate timing for invasive mechanical ventilation to facilitate other lung protective strategies, including prone position, and therefore avert further deterioration and patient self-inflicted lung injury.7172
A higher rate of difficult or failed tracheal intubation is evident in pregnant patients.73 Additionally, owing to the decreased respiratory reserve, pregnant women are at increased risk of oxygen desaturation during general anesthesia induction,74 which may be compounded in women with severe covid-19 infection. Therefore, it is essential to optimize first pass intubation success rates. International consensus guidelines for managing the airway in patients with covid-19 recommend adopting strategies to enable successful airway management (“safe, accurate, and swift”).75 These strategies include evaluating the “most appropriate” clinician to manage the airway. The most appropriate person is based on factors such as the available clinician’s airway experience and expertise, and the predicted difficulty of airway management.
Positioning
Use of the prone position to improve oxygenation is now an established treatment strategy in patients with severe covid-19. In a prospective collaborative meta-trial of six randomized controlled open label superiority trials, adults (excluding pregnant women) who required respiratory support with high flow nasal cannula for acute hypoxemic respiratory failure owing to covid-19 were randomly assigned to awake prone positioning or standard care. The primary composite outcome was treatment failure, defined as the proportion of patients intubated or dying within 28 days of enrolment. Treatment failure occurred in 40% of patients assigned to awake prone positioning and 46% of patients assigned to standard care (relative risk, RR 0.86, 95% CI 0.75 to 0.98). Data about the prone position in pregnant women are limited to case reports, but are reassuring. Routine indications and contraindications should apply, although it may be appropriate to avoid the position in the immediate postoperative period after cesarean birth. In the third trimester, prone positioning may be more challenging technically, and the lateral decubitus position may be better tolerated76; the risks and benefits of delivery before prone positioning should be considered. When undertaken, ensure adequate padding above and below the gravid uterus to offload the uterus and avoid aortocaval compression.77 Fetal monitoring during periods in the prone position may be technically challenging, but can be undertaken if required.78
In a case series of obstetric patients with severe covid-19 infection, 13 patients had prone positioning during their care, with 49 proning sessions of median duration 16 hours (interquartile range 2.8, range 1 to 18). No proning sessions were terminated owing to maternal hemodynamic or respiratory instability, or fetal intolerance. One patient developed uterine contractions while prone, which resolved when the woman was returned to the supine position. The authors reported that in some cases, maintaining continuous fetal monitoring while in the prone position required an early return to the supine position.76 This emphasizes the importance of multidisciplinary discussion to assess whether continuous fetal monitoring is needed if its application denies a pregnant woman the benefits of the prone position.
Extracorporeal membrane oxygenation
Early in the pandemic, ECMO was identified as having a role in managing refractory hypoxemia unresponsive to conventional care. In a retrospective cohort study, the Extracorporeal Life Support Organization Registry reported outcomes of pregnant or peripartum women with covid-19 supported with veno-venous ECMO (VV-ECMO).79 The primary outcome was survival to hospital discharge, and secondary outcomes were complications related to ECMO in the pregnant or peripartum cohort. In the cohort, 1180 adult female patients were supported with VV-ECMO for covid-19, of whom 100 were pregnant or peri partum. The pregnant or peripartum group was more likely to survive to hospital discharge (84% v 51.5%; overlap propensity score weighted OR 1.18; 95% CI 1.10 to1.27) and had fewer renal complications related to ECMO (overlap propensity score weighted OR 0.90; 95% CI 0.84 to 0.97). Consensus recommendations from the UK and US suggest that ECMO be offered to selected patients with acute severe respiratory failure caused by covid-19,80 and the same criteria for referral should be used for pregnant and postpartum women as for non-pregnant patients (box 1).8081 The rapid report from the UK Confidential Enquiry into Maternal Deaths during the pandemic found several examples of women who were inappropriately deemed ineligible for ECMO.26 This occurred particularly when women developed air leaks (eg, pneumomediastinum or subcutaneous emphysema) as a consequence of high inspiratory effort. Pregnant and postpartum women with severe covid-19 should be referred early to a severe respiratory failure/ECMO center to avert delays in lung protective ventilation or extracorporeal therapies. The combination of reduced lung volumes, increased cardiac output (ie, increased effective shunt fraction), and concerns around proning associated with the excellent prognosis and response to extracorporeal support of pregnant women should further encourage early engagement with ECMO centers. Special considerations may be required in terms of ECMO configuration, immunomodulation during ECMO, and obstetric care, which require multidisciplinary discussion and again emphasize the importance of managing pregnant women in centers where all these disciplines are available.
Indications for use of ECMO in severe respiratory failure80
Criteria for referral for ECMO
Potentially reversible severe respiratory failure (eg, PaO2/FiO2 of <6.7 kPa for ≥3 h or PaO2/FiO2 of <10.0 kPa for ≥6 h)81
Lung injury score of 3 or higher82
Uncompensated hypercapnia with a pH of 7.20 or higher, despite a respiratory rate of more than 35 breaths/min, or owing to life threatening airway disease (eg, asthma, airway trauma, or air leak)14
Criteria for considering ECMO
Unsuccessful trial of ventilation in the prone position for six hours or more (unless contraindicated)
Unsuccessful optimal respiratory management with lung protective ventilation after discussion with an ECMO center
Obstetric care
Concurrent medication
Covid-19 infection may be associated with thrombocytopenia,83 thus aspirin prescribed for pre-eclampsia prophylaxis should be withheld during the period of illness to reduce the risk of bleeding if platelets <50 ×109/L.8 Aspirin irreversibly inhibits COX-1, inducing a longlasting functional defect in the platelets. Its effect lasts approximately one week after discontinuing treatment.
Mode of birth and pregnancy outcomes
Most women infected with covid-19 show no evidence of respiratory compromise and should be allowed to recover from the infection and proceed as usual through the remainder of their pregnancy.84 If a woman is admitted to hospital for covid-19 during pregnancy, regular ultrasound screening for fetal growth should be performed from 28 weeks onwards, as per the local policy on routine screening for fetal growth restriction.
Covid-19 status alone is not an indication for cesarean birth, and the usual indications should guide the mode of birth. Maternal covid-19 infection is associated with an increased risk of cesarean birth (50% compared with 29% in controls) regardless of symptom status, with half of the additional cesarean births directly as a result of expedited delivery owing to maternal compromise.10 Some studies suggest that in women with symptomatic covid-19, an increased risk of fetal compromise may be seen in active labor; 23% of cesarean births in women admitted with symptomatic covid-19 in a UK national cohort were because of fetal compromise.10 However, poor reporting of the indication for cesarean birth in many studies makes it difficult to fully separate any iatrogenic effect from the true impact of covid-19.1
Women with symptomatic suspected or confirmed covid-19 should be advised to undergo labor and give birth in an environment that enables multidisciplinary care (obstetric, physician, anesthetic, midwifery, and neonatology) for the woman and her baby. They should be offered continuous electronic fetal monitoring during labor.
In cases where the mother’s condition deteriorates, individualized multidisciplinary assessment about the mode of birth should consider maternal preference and gestation. Studies have consistently identified that the preterm birth rate in women with symptomatic covid-19 is approximately three times higher than the background rate, predominantly owing to iatrogenic preterm births.1
Preterm birth is a leading cause of neonatal morbidity and mortality. Potential maternal benefits of expediting delivery must be carefully balanced against the risk to the fetus of iatrogenic prematurity. Multiple case reports describe women with severe covid-19 infection in the first and second trimesters receiving critical care, including mechanical ventilation and ECMO, and recovering to complete the remainder of their pregnancies.8586 In cases where preterm birth is considered necessary, magnesium sulfate therapy should be administered for fetal neuroprotection up to 29+6 weeks’ gestation and considered up to 33+6 weeks’ gestation.87 Administration of steroids (either dexamethasone or betamethasone) for fetal lung maturity should be considered prior to delivery before 34+6 weeks’ gestation.888
No evidence exists of an increased risk of congenital abnormality or fetal loss before 20 weeks in women who have contracted covid-19 in pregnancy. In several more recent studies of women with laboratory confirmed SARS-CoV-2 infection, however, the risk of stillbirth appears significantly increased compared with women without infection; this is particularly evident since the delta variant became predominant.241784 Proposed mechanisms include impaired placental function secondary to the infection.
Reassuringly, no evidence suggests increased rates of neonatal morbidity in babies born at term. In addition, babies born to mothers who have tested positive for covid-19 are unlikely to contract the virus, supporting the practice of not separating mother and baby at birth.89
Transplacental transmission of immunoglobulin G antibodies against covid-19 has been shown in umbilical cord blood samples from infected mothers.90 At present, the duration of their existence and the extent to which they confer passive immunity remains unclear.
A multicenter international cohort study investigated 30 day mortality and pulmonary complications in patients with perioperative SARS-CoV-2 infection.91 The authors found higher 30 day mortality in elective and emergency surgical patients, respectively, with around half of patients experiencing postoperative pulmonary complications. Therefore, current recommendations are that planned surgery should not be scheduled within seven weeks of a diagnosis of SARS-CoV-2 infection unless outweighed by the risk of deferring surgery, or clinical priority, or during the period that a patient may be infectious (10 days after mild/moderate disease and 15-20 days after severe disease) for the protection of staff. However, the potential to delay or postpone cesarean birth or induce labor is limited. In a woman who has recovered from recent SARS-CoV-2 infection, a personalized assessment should determine whether it is feasible or beneficial to delay a planned cesarean birth or induction of labor.
Occasionally, later in the third trimester, early delivery of the baby may result in improved respiratory system compliance, and therefore delivery may lead to reduced oxygen requirements and improvements in the mother’s condition. Decisions regarding timing, place, and mode of delivery should be taken by a multidisciplinary team including obstetricians, physicians, anesthetists, and intensivists experienced in the care of covid-19 in pregnancy, and ideally this should take place in consultation with centers with experience and expertise in all these specialties.
Postpartum care
Skin-to-skin contact after birth, along with breastfeeding, improves maternal-infant bonding and perinatal mental health outcomes (fig 6).89 Vertical transmission, although reported, is uncommon,89 and rates of infection are no greater when a baby is born vaginally, has skin-to-skin contact (is dried immediately after birth and laid directly on the mother’s bare chest for at least an hour or until after the first feed), is breastfed, or remains in close contact with a mother who has covid-19.92 As vertical transmission of covid-19 is exceptionally rare and the risk of severe infection in neonates is small, the World Health Organization encourages covid positive mothers and their babies to be allowed to remain together, promoting breastfeeding using sensible hygiene precautions.93 Despite best efforts, in some women periods of separation from their newborn will be unavoidable. For such women and for those who have been put under severe mental stress because of being very unwell during their pregnancy, a postnatal birth reflections service, perinatal mental health, or clinical psychology team may be of benefit.

Facilitate contact for mother and neonate, even in the ICU setting, to support maternal-infant bonding
{kind=link}
Prognosis of covid-19 in pregnancy
The prognosis of covid-19 varies according to trimester of infection, with data from the Scottish national cohort study showing rates of admission to hospital varying from 3% to 16% with infection in the first trimester, to 7-28% in the second trimester, and 28-54% in the third.17 Outcomes for women who are not admitted to hospital appear to be good,17 although pregnant women with covid-19 are reported to be at increased risk of developing pre-eclampsia compared with women giving birth without covid-19.194 It is, as yet, unclear whether an independent association exists, or whether the association is caused by common risk factors. Results from the INTERCOVID prospective longitudinal study suggest the association is independent of any risk factors (including covid-19 severity) and pre-existing conditions.94 Pre-eclampsia and covid-19 were associated independently of, and in additive fashion with, preterm birth, perinatal morbidity and mortality, as well as adverse maternal outcomes. It was therefore concluded that clinicians should be alert to women with pre-eclampsia being a particularly vulnerable group with regard to the risk of covid-19.
Between one in six and one in 12 pregnant women admitted to hospital with symptomatic covid-19 in pregnancy (as opposed to an incidental diagnosis on admission screening) are admitted to an intensive care unit.2 Case fatality rates among those admitted vary widely, according to study design and setting; rates of up to 1%, depending on the period, have been reported among the national cohort of women admitted to hospital with symptomatic covid-19 in pregnancy in the UK.2 Up to 17 January 2022, 263 deaths among 160 873 pregnant women with covid-19 had been reported in the US, a rate of 16 per 10 000 pregnant women with covid-19.9 The odds of mortality are threefold higher among pregnant women with covid-19 compared with pregnant women without covid-19 (OR 2.85, 95% CI 1.08 to 7.52).1
As of 17 January 2022, the Centers for Disease Control and Prevention reported that about 10% of pregnant women with covid-19 gave birth preterm.9 Among women admitted to hospital with symptomatic covid-19 in pregnancy, rates of preterm birth are more than 20%, with most of the excess resulting from iatrogenic deliveries.2 Perinatal mortality rates are reported to be more than fourfold higher among pregnant women with SARS-CoV-2 within 28 days of giving birth, compared with pregnant women without SARS-CoV-2.17
Few data yet exist on longer term outcomes of covid-19 in pregnancy for either women or their infants, but research is ongoing. However, given the known long term neurodevelopmental and other impacts of preterm birth, it is clear that long term adverse sequelae will result.
Covid-19 vaccination in pregnancy
Covid-19 vaccines have no biologically plausible mechanism by which to cause harm in the periconception period, throughout gestation, or during breastfeeding. As such, professional organizations, including the American College of Obstetricians and Gynecologists, the Royal College of Obstetricians and Gynaecologists, and Royal College of Midwives in the UK, strongly endorse the vaccination of pregnant women, based on their age and clinical risk group, in line with non-pregnant women. Substantial data are available on safety for messenger RNA (mRNA) vaccines in pregnancy, and pregnant women should be advised that the vaccine prevents severe illness, and that the benefits to mother and baby far outweigh any—largely theoretical—risks.849596 Data for fetal outcomes are reassuring, with rates of preterm birth, small-for-gestational age, congenital anomaly, pregnancy loss, and stillbirth not being increased above the background population.9596 A recent analysis in six European countries showed that almost all pregnant women admitted to intensive care units with covid-19 in the latter half of 2021, when vaccination was universally available, were unvaccinated.97 A national study from Scotland showed that all babies who were stillborn or died in the neonatal period after maternal covid-19 were born to mothers who had not been vaccinated.17 These studies give clear evidence of the strong protection vaccination affords against the severest outcomes of covid-19 for both mother and baby. Clinicians should strongly encourage pregnant women to accept vaccination, signposting them to reliable information.
Emerging treatments
New, innovative, and emerging treatments have become available to treat covid-19, but very few, if any studies have included pregnant women. This is a concern and needs to be addressed if we are to provide equitable and fair treatment to pregnant women, as we do other patient populations.98 While acknowledging concerns regarding medication safety in pregnancy, relative safety can often be inferred through scientific appraisal of the mechanism of action of the study medication and looking in the literature for the use of the study medication (or a similar class of medication) to treat other diseases. Ultimately, if a pregnant woman is unwell with covid-19, the risks to the baby and mother from the disease itself (hypoxia, hypovolemia, premature delivery) are likely to be as harmful, if not more so, than medication given to treat.
Emerging covid-19 studies that have included pregnant women include the RECOVERY trial. At present RECOVERY includes pregnant women in the high dose steroids arm, the sotrovimab arm, and the paxlovid arm. Baricitinib, a Janus kinase inhibitor that inhibits the endocytosis of SARS-CoV-2 into pulmonary cells, has shown a proportional reduction in mortality of 13% in the RECOVERY trial, and when combined with results from other studies, a 20% overall reduction in mortality.99 Limited information is available about the safety of baricitinib in pregnancy. In a case report describing a patient with rheumatoid arthritis exposed to baricitinib from conception to 17 weeks’ gestation, a healthy infant was born at 38 weeks. Tofacitinib, another Janus kinase inhibitor, has limited data, with approximately 60 exposed pregnancies reported in a small number of uncontrolled case series100 and a case report,101 for which the pregnancy outcomes are reassuring. Thus, although data around the safety of Janus kinase inhibitors in pregnancy are limited, these treatments remain a therapeutic option worthy of further studies.
Clinical trials of camostat mesilate (a serine protease inhibitor) and sargramostim (a recombinant human granulocyte-macrophage colony stimulating growth factor) are also emerging. To date, no pregnancy exposure data, either human or animal, exist for these medications.102
Guidelines
To inform this review, we considered resources from the American College of Obstetricians and Gynecologists, the Society for Maternal-Fetal Medicine, the Royal College of Obstetricians and Gynaecologists, and the Society of Obstetricians and Gynecologists of Canada. All sources reference other guidance—for example, National Institutes of Health covid-19 treatment guidelines, and are continually being revised as evidence emerges. Considering the emerging evidence, some guidance is framed as frequently asked questions (FAQs), rather than formal guidance documents. Aspects of these FAQs and/or formal guidance documents changed on several occasions during the drafting of this article, and we therefore advise consultation of current sources for individual detail (box 2).
Selected national guidance on management of covid-19 in pregnancy
American College of Obstetricians and Gynecologists: https://www.acog.org/clinical-information/physician-faqs/covid-19-faqs-for-ob-gyns-obstetrics
National Institutes of Health: https://www.covid19treatmentguidelines.nih.gov
Royal College of Obstetricians and Gynaecologists: https://www.rcog.org.uk/guidance/coronavirus-covid-19-pregnancy-and-women-s-health/coronavirus-covid-19-infection-in-pregnancy/
Society for Maternal-Fetal Medicine: https://www.smfm.org/covidclinical
Society of Obstetricians and Gynecologists of Canada: https://sogc.org/en/-COVID-19/en/content/COVID-19/COVID-19.aspx?hkey=4e808c0d-555f-4714-8a4a-348b547dc268
Conclusion
Pregnant women with covid-19 are at greater risk of severe disease than their non-pregnant peers. The basic principles of diagnosis and management are the same as for non-pregnant patients and it is important that pregnant women are not denied investigations or treatment inappropriately. A multidisciplinary, expert team approach is essential to ensure all facets of care are optimized. Earlier and rapid escalation to the appropriate teams is needed to continue to improve outcomes for both women and their babies. Corticosteroid therapy should be modified during pregnancy to use non-fluorinated glucocorticoids. Il-6 inhibitors and monoclonal antibodies, together with specific antiviral therapies, may also be considered. Prophylaxis against venous thromboembolism is particularly important. Women may require respiratory support with oxygen, non-invasive ventilation, ventilation in a prone position (either awake or during invasive ventilation), intubation and ventilation, and ECMO. Pregnancy is not a contraindication for any of these supportive therapies and the criteria for providing these therapies are the same as in the general population. In some clinical situations, particularly later in the third trimester, early delivery of the baby may facilitate improvement of the maternal condition. Decisions regarding time, place, and mode of delivery should be taken with a multidisciplinary approach, ideally, in a center with appropriate expertise. Vaccination for covid-19 is of paramount importance in this population and should be strongly recommended, with appropriate signposting to reliable information. Future trials of vaccines and therapies should enable the inclusion of pregnant participants if equitable and fair treatment is to be provided to the pregnant population.
Research questions
What is the appropriate dose of low molecular weight heparin for venous thromboembolism prophylaxis in covid-19 in pregnancy?
What is the efficacy of prednisolone and/or methylprednisolone in preventing severe outcomes of covid-19 in pregnancy?
How effective is prone positioning in the treatment of pregnant women with covid-19? How can the prone position be used more effectively in pregnant women?
What are the long term outcomes of covid-19 in pregnancy for women and their children?
How patients were involved in the creation of this article
This manuscript has been informally peer reviewed by a patient who was infected with SARS-CoV-2 during pregnancy and admitted to hospital under the care of three of the authors. The patient required admission to intensive care and ECMO support; cesarean section was undertaken at 32 weeks’ gestation owing to maternal compromise.
Following review of the manuscript, the patient emphasized the importance of communication and collaboration of the multidisciplinary team. She also described eloquently the emotions involved in delivering a preterm baby under such circumstances.
“A mother’s instinct and concern is the health and protection of their baby. It consumed my every waking hour. Who is looking after her? How is she? When can I meet her? All the ‘firsts’ I was missing: first nappy, first feed, coming off oxygen, etc. My baby came first and it physically hurt my heart not to be able to meet her. Communication was priceless.
“The first time I met her was gut wrenching … will she take to me? Will I know what to do? But with support from a fantastic team behind me, meeting my baby for the first time was everything and more. The relief was immense and gave me fire in my belly to get better and to have her in my arms for the rest of my life.”
Footnotes
Contributorship: All authors planned the overall content of the article. MN, MK, and KH conducted the literature reviews. MN and CNP wrote the first draft of the article. All authors edited specific sections and revised the whole article for intellectual content. MK and CNP are guarantors.
Competing interests: We have read and understood the BMJ policy on declaration of interests and declare the following interests: MK reports grants from the National Institute for Health Research; CNP reports grants and speaker fees from UCB unrelated to covid-19 and speaker fees from Sanofi and Alexion pharma; KH reports he is a local principal investigator for the Pfizer-BioNTech maternal SARS CoV-2 RNA Vaccine study (ClinicalTrials number NCT04754594). All other authors report none.
Provenance and peer review: commissioned; externally peer reviewed.
The photo in figure 6 is included with permission from patient.