Psychological interventions for chronic, non-specific low back pain: systematic review with network meta-analysis
BMJ 2022; 376 doi: https://doi.org/10.1136/bmj-2021-067718 (Published 30 March 2022) Cite this as: BMJ 2022;376:e067718
- Emma Kwan-Yee Ho, doctoral student1 2,
- Lingxiao Chen, doctoral student2,
- Milena Simic, associate professor1,
- Claire Elizabeth Ashton-James, associate professor3 4,
- Josielli Comachio, research assistant1,
- Daniel Xin Mo Wang, research assistant1,
- Jill Alison Hayden, associate professor5,
- Manuela Loureiro Ferreira, professor2,
- Paulo Henrique Ferreira, professor1
- 1Sydney Musculoskeletal Health, School of Health Sciences, Charles Perkins Centre, Faculty of Medicine and Health, University of Sydney, Sydney, NSW, Australia
- 2Sydney Musculoskeletal Health, The Kolling Institute, School of Health Sciences, Faculty of Medicine and Health, University of Sydney, Sydney, NSW, Australia
- 3Sydney Medical School, Faculty of Medicine and Health, University of Sydney, Sydney, NSW, Australia
- 4Pain Management Research Institute, Kolling Institute, University of Sydney, Sydney, NSW, Australia
- 5Department of Community Health and Epidemiology, Faculty of Medicine, Dalhousie University, Halifax, NS, Canada
- Correspondence to: E Ho emma.ho{at}sydney.edu.au (or @EmmaK_Ho on Twitter)
- Accepted 1 February 2022
Abstract
Objective To determine the comparative effectiveness and safety of psychological interventions for chronic low back pain.
Design Systematic review with network meta-analysis.
Data sources Medline, Embase, PsycINFO, Cochrane Central Register of Controlled Trials, Web of Science, SCOPUS, and CINAHL from database inception to 31 January 2021.
Eligibility criteria for study selection Randomised controlled trials comparing psychological interventions with any comparison intervention in adults with chronic, non-specific low back pain. Two reviewers independently screened studies, extracted data, and assessed risk of bias and confidence in the evidence. Primary outcomes were physical function and pain intensity. A random effects network meta-analysis using a frequentist approach was performed at post-intervention (from the end of treatment to <2 months post-intervention); and at short term (≥2 to <6 months post-intervention), mid-term (≥6 to <12 months post-intervention), and long term follow-up (≥12 months post-intervention). Physiotherapy care was the reference comparison intervention. The design-by-treatment interaction model was used to assess global inconsistency and the Bucher method was used to assess local inconsistency.
Results 97 randomised controlled trials involving 13 136 participants and 17 treatment nodes were included. Inconsistency was detected at short term and mid-term follow-up for physical function, and short term follow-up for pain intensity, and were resolved through sensitivity analyses. For physical function, cognitive behavioural therapy (standardised mean difference 1.01, 95% confidence interval 0.58 to 1.44), and pain education (0.62, 0.08 to 1.17), delivered with physiotherapy care, resulted in clinically important improvements at post-intervention (moderate quality evidence). The most sustainable effects of treatment for improving physical function were reported with pain education delivered with physiotherapy care, at least until mid-term follow-up (0.63, 0.25 to 1.00; low quality evidence). No studies investigated the long term effectiveness of pain education delivered with physiotherapy care. For pain intensity, behavioural therapy (1.08, 0.22 to 1.94), cognitive behavioural therapy (0.92, 0.43 to 1.42), and pain education (0.91, 0.37 to 1.45), delivered with physiotherapy care, resulted in clinically important effects at post-intervention (low to moderate quality evidence). Only behavioural therapy delivered with physiotherapy care maintained clinically important effects on reducing pain intensity until mid-term follow-up (1.01, 0.41 to 1.60; high quality evidence).
Conclusions For people with chronic, non-specific low back pain, psychological interventions are most effective when delivered in conjunction with physiotherapy care (mainly structured exercise). Pain education programmes (low to moderate quality evidence) and behavioural therapy (low to high quality evidence) result in the most sustainable effects of treatment; however, uncertainty remains as to their long term effectiveness. Although inconsistency was detected, potential sources were identified and resolved.
Systematic review registration PROSPERO CRD42019138074.
Introduction
Low back pain (LBP) describes pain, muscle tension, or stiffness localised below the costal margin and above the inferior gluteal folds, with or without leg pain. LBP is defined as chronic when it persists for more than 12 weeks. Psychological factors have an important role in an individual’s experience of LBP and its impact on their functioning and quality of life. Fear avoidance beliefs, depression, anxiety, catastrophic thinking, and familial and social stress are highly prevalent in adults with chronic LBP1 and can increase the risk of physical disability,23 manifesting as reduced functional capacity, avoidance of usual activities including work, and impaired societal and recreational participation.4 Fear avoidance beliefs can also mediate the relation between pain and disability in individuals with LBP,56 and have an important influence on physical health related quality of life and health service usage in this population.7 Consequently, consideration of psychological factors might be important in the management of LBP.8
Psychological interventions for chronic pain conditions commonly aim to reduce pain related distress and disability by changing patients’ negative beliefs, behaviours, and attitudes through a combination of principles and strategies informed by psychological theories. Several systematic reviews have examined the effectiveness of psychological interventions for chronic, non-specific LBP.9101112131415 Yet, previous reviews have mainly focused on a small selection of psychological approaches for chronic LBP (that is, cognitive behavioural therapy and behavioural therapies), neglecting more recently developed psychological interventions (that is, cognitive functional therapy and acceptance and commitment therapy). Importantly, previous reviews have conducted only independent pairwise meta-analyses, and to our knowledge, no attempts have been made to synthesise the results cohesively. Ultimately, the comparative effectiveness and safety of the wider collection of psychological interventions available for managing chronic LBP is unknown, representing an important gap in the evidence.
Most clinical practice guidelines endorse the use of psychological treatments for chronic LBP.16 However, existing guidelines typically provide generic or incomplete recommendations. Cognitive behavioural therapy is the most frequently recommended psychological approach,16 often without mention of evidence for other forms of psychological interventions.171819 Some guidelines list a range of psychological interventions that might be beneficial for chronic LBP.19202122 However, making decisions about psychological interventions for LBP is fraught with difficulty owing to lack of information about which psychological interventions are most effective to obtain a specific clinical outcome of interest and a paucity of evidence for the comparative longevity of intervention outcomes. Examining the comparative effectiveness and safety of the wide range of available psychological interventions for chronic LBP might help to improve the clarity of guideline recommendations and better support clinicians and patients in treatment decision making.
In this systematic review, we used a network meta-analysis design (NMA) to investigate the comparative effectiveness of different types of psychological interventions for improving physical function, pain intensity, fear avoidance, health related quality of life, and intervention compliance in people with chronic, non-specific LBP. We also investigated the comparative safety of psychological interventions for this population. In contrast to traditional pairwise meta-analysis, NMA involves the synthesis of direct and indirect evidence to enable simultaneous comparison and ranking of numerous competing interventions within one coherent treatment network.
Methods
Study design
This systematic review with NMA was reported in accordance with the PRISMA statement for systematic reviews23 and the PRISMA extension for NMA (PRISMA-NMA).24 The protocol was registered on PROSPERO (registration No CRD42019138074) and the protocol paper was peer reviewed and published in BMJ Open.25 The systematic review team consisted of physiotherapists (EK-YH, JC, DXMW, MS, MLF, and PHF), a medical doctor (LC), a psychologist (CEA-J), and a chiropractor (JAH). These reviewers are experienced in the design and conduct of systematic reviews.
Data sources
We searched Medline, Embase, PsycINFO, Cochrane Central Register of Controlled Trials, Web of Science, SCOPUS, and CINAHL via OVID from database inception until 31 August 2020, and updated our search on 31 January 2021. Our search combined an exhaustive list of concepts, language, and keywords for randomised controlled trial, LBP, and psychological interventions (supplementary A). We also searched reference lists of relevant systematic reviews and clinical guidelines.
Study selection
Types of studies
We included parallel and cluster randomised controlled trials, and the first phase of crossover randomised controlled trials, which had been published in peer reviewed journals. We did not restrict our studies by length of follow-up. The search excluded observational studies, non-randomised trials, short reports, research letters, conferences abstracts, or studies that had not been published as full length articles in peer reviewed scientific journals. In accordance with the Cochrane Handbook,26 cluster randomised controlled trials were included only when study results accounted for the cluster design (eg, data analysed at the level of allocation).
Types of participants
We included studies of people aged 18 years and older,experiencing chronic, non-specific LBP, with or without the presence of leg pain. We defined chronic, non-specific LBP according to guidelines from the UK National Institute for Health and Care Excellence as pain in the back between the bottom of the rib cage and buttocks crease with no known pathoanatomical cause, for more than 12 weeks in duration.1727 The analysis excluded studies of participants with serious pathologies (eg, spinal stenosis, malignancy, trauma, vertebral fracture, infection, and inflammatory disorders). We included studies involving a combination of populations with acute, subacute, or chronic LBP, provided that more than 50% of participants had chronic LBP and that the results were reported separately for the chronic LBP subgroup. The analysis also included studies of participants who had chronic LBP combined with other chronic pain conditions, provided that more than 50% of participants reported a diagnosis of chronic LBP and that the results were reported separately for the chronic LBP subgroup. Disagreements were resolved by consensus among systematic reviewers (EK-YH, JC, DXMW, PHF).
Types of interventions
We included studies comparing psychological interventions (independently or combined with another treatment) with any comparison interventions. We replicated the definition provided by Hoffman et al10 by defining psychological interventions as interventions conceived by the authors of the study as being a psychological intervention. Our analysis expanded on this definition by further including interventions clearly based on any of the following approaches: cognitive behavioural therapeutic strategies , mindfulness based stress reduction, acceptance and commitment therapy, cognitive functional therapy, health coaching, biofeedback (delivered with a therapeutic intent to promote muscle relaxation), pain education, and counselling directly using principles of psychological theory. Examples of cognitive behavioural strategies were relaxation, graded exposure (desensitisation), imagery (distraction), goal setting, and operant conditioning. We also included studies of combined psychological approaches, defined as interventions containing two or more psychological approaches delivered together, with or without additional non-psychological co-interventions. The non-psychological co-interventions or comparison interventions identified by our search strategy had no restrictions, provided that the psychological, non-psychological co-intervention (if present), and comparison interventions could be classified into our initial prespecified treatment nodes (supplementary B). Citations identified by our search strategy were managed using Endnote X928 and screened using Covidence.29 Two pairs of reviewers (EK-YH and JC, JC and DXMW) independently screened eligibility in two stages: citation titles and abstracts, and full text. Disagreements were resolved by consensus among systematic reviewers (involving physiotherapists (EK-YH, JC, DXMW, and PHF) and the psychologist (CEA-J)).
Outcome measures
The primary outcomes were physical function and pain intensity of the lower back, which were continuous outcomes. The secondary outcomes were fear avoidance, health related quality of life, intervention compliance, and safety. We defined fear avoidance as fear of pain and consequent avoidance of movement. Intervention compliance was assessed as the proportion of participants who completed their assigned intervention (psychological or comparison) during the intervention period. We defined safety as the proportion of participants who had at least one adverse effect during the intervention period. Adverse effects were broadly defined as any adverse event, side effect, complication, or event resulting in discontinuation of treatment, which was associated with the intervention (psychological or comparison) under investigation. Safety was assessed in studies that were included in the NMA for either of the primary outcomes of this systematic review.
Existing outcome data for all available follow-up time points were extracted for all outcomes of interest. We classified data according to the following intervals: pre-intervention (that is, baseline); post-intervention (that is, at the end of treatment or <2 months post-intervention); short term treatment sustainability (from ≥2 to <6 months post-intervention); mid-term treatment sustainability (from ≥6 to <12 months post-intervention); and long term treatment sustainability (≥12 months post-intervention). An NMA was conducted at each time point separately. If two or more follow-up assessments occurred within a given time point, we analysed data that were assessed at the time point closest to the lower limit of the respective category. The primary endpoint for all analyses was post-intervention.
Data extraction
Two reviewers (JC and DXMW) independently extracted all available data for publication (eg, publication year and funding), study design (eg, number of participants randomised and duration of follow-up), participants (eg, age, sex, body mass index, race or ethnic minority, comorbidities, and socioeconomic status (that is, education and income levels)), and intervention characteristics (eg, key components of the psychological and comparison interventions, intervention dosage and frequency, and intervention duration), as well as relevant outcome data. Disagreements were resolved by consensus among systematic reviewers (JC, DXMW, EK-YH, PHF). We contacted 21 authors of studies that might have met our inclusion criteria to request information or data to determine suitability for inclusion in our systematic review (eg, availability of data for chronic, non-specific LBP subgroup only, data for sample characteristics, and missing outcome data). In total, 12 (57%) of 21 authors provided the necessary information or data.
For studies reporting two or more measures of physical function at a given time point, we used the following hierarchy for extraction: Oswestry Disability Index, Roland Morris Disability Questionnaire, Core Outcome Measures Index, Quebec Back Pain Disability Index, rating scales for disability within a composite measure of physical function (eg, 12 or 36 item short form (SF-12 or SF-36)), and other measurement tools.3031 For studies reporting two or more measures for pain intensity at a given time point, we used the following hierarchy for extraction: Numeric Rating Scale, Visual Analogue Scale, rating scale for pain intensity from a composite measure of pain intensity (eg, McGill Pain Questionnaire), and other measurement tools.3031 For studies reporting two or more measures for pain intensity at a given time point, we extracted data according to the following order: average pain intensity (preferred), worst pain intensity, and alternative measures of pain intensity. For studies reporting two or more measures of fear avoidance at a given time point, we used the following hierarchy for extraction: Fear Avoidance Beliefs Questionnaire; Pain Catastrophising Scale; Tampa Scale of Kinesiophobia; Fear of Pain Questionnaire; rating scales of fear avoidance from a composite measure of fear avoidance; and other measurement tools.32 If authors reported Fear Avoidance Belief Questionnaire scores, we extracted data according to the following hierarchy: physical activity scale, work scale, overall score. If authors only provided an overall score for the Fear Avoidance Beliefs Questionnaire, we contacted them for the physical activity (preferred) or work subscores. For studies measuring health related quality of life at a given time point, we used the following hierarchy for extraction: Patient-Reported Outcomes Measurement Information System-Global Health-10; EuroQoL-5D; SF-12 or SF-36 (physical component summary subscore); SF-12 or SF-36 (mental component summary subscore); SF-36 (overall score); Nottingham Health Profile 3031; rating scale from a composite measure of health related quality of life; and other measurement tools.
To assess intervention compliance, we extracted the number of participants who completed their assigned intervention, as reported by the study authors. If this information was not available, we subtracted the sum of the reported number of participants who did not commence their assigned intervention and those who commenced but discontinued their assigned intervention, from the total number of participants allocated to the respective intervention group. Studies that did not report any of the previously mentioned information clearly were not included in the NMA for intervention compliance. In accordance with the protocol, we initially assumed intervention compliance for no intervention was 100%.25 However, we decided that this assumption was not clinically meaningful and would bias effect estimates. Therefore, we excluded the nointervention treatment node from our NMA for intervention compliance.
Risk of bias in individual studies and confidence in the evidence
After pilot testing, two reviewers (JC and DXMW) independently assessed risk of bias for the relevant outcomes, only in studies included in the NMA, using the licensed Excel tool to implement the revised Cochrane risk-of-bias 2 tool for randomised trials.3334 An overall risk of bias judgment (low risk of bias, some concerns, or high risk of bias) was made based on five domain level judgments, as described in Sterne et al.35 Disagreements were resolved through a third reviewer (EK-YH). Confidence in the cumulative evidence was evaluated using the Confidence in NMA (CINeMA) framework,36 a web application of the Grading of Recommendations Assessment, Development, and Evaluation ratings approach. A description of the reasons for downgrading confidence ratings has been provided in supplementary K.
Treatment node classification
The final network consisted of 17 treatment nodes (table 1, supplementary B). Examples of interventions or approaches that were classified into the respective treatment nodes have been described in the published protocol paper.25 Psychological interventions were clustered into six nodes: behavioural interventions, cognitive behavioural therapies, mindfulness, counselling, pain education, and combined psychological approaches (that is, the delivery of two or more psychological approaches together, in the absence of a non-psychological co-intervention). Comparison interventions were classified as: physiotherapy care, general practitioner care, advice, no intervention, and usual care. Each psychological intervention node, delivered with physiotherapy care as a co-intervention, formed a separate treatment node.
Final treatment nodes included in network meta-analysis
Physiotherapy care was the reference comparison intervention. Physiotherapy care was selected because exercise and passive therapies, which are frequently prescribed or used by physiotherapists, were the most frequently investigated comparison interventions in the included studies and because exercise is the most commonly endorsed treatment approach for managing chronic LBP.816 To explore potential heterogeneity within the physiotherapy care node, we identified all studies included in the review that involved physiotherapy care (as a non-psychological co-intervention or a comparison intervention) in at least one of the intervention arms. Then, we delineated between the number of studies in which the physiotherapy care node consisted of exercise alone, passive therapy alone, or exercise delivered with passive therapy.
Statistical analysis
We conducted quantitative analysis for physical function, pain intensity, fear avoidance, and intervention compliance. For both traditional pairwise meta-analyses and NMA, we estimated random effects using the restricted maximum likelihood method, and derived 95% confidence intervals using the Hartung-Knapp-Sidik-Jonkman approach.42 We performed traditional pairwise meta-analyses for all direct comparisons with at least two studies available, and random effects NMA with a frequentist approach to simultaneously combine direct and indirect evidence. We assumed that the heterogeneity variance across different comparisons within the NMA model were the same. We estimated the mean rank and relative treatment rankings for each intervention node according to the surface under the cumulative ranking curve (SUCRA) values. We produced rankograms for the primary outcomes at each time point of analysis.
Many studies only reported change from baseline scores and did not provide outcome scores at post-intervention or follow-up time points. Consequently, to maximise the number of studies included in the NMA, we converted mean baseline and outcome scores for each intervention group, at each relevant time point, into scores of change from baseline with the accompanying measures of variance. Change scores were calculated in accordance with formulas provided in the Cochrane Handbook.26 We calculated change from baseline means by subtracting outcome means from baseline means, and calculated change from baseline standard deviations by using the formula provided in the handbook, assuming a correlation coefficient (r) of 0.50.26 We selected r=0.50 as a conservative approximation of estimates presented by Suzuki et al,43 who examined the correlation between changes in pain intensity in people with chronic LBP relative to changes in various clinical outcomes after treatment. Continuous outcomes (that is, physical function, pain intensity, fear avoidance) were measured using different rating scales; therefore, we converted outcomes to standardised mean differences (SMD) and 95% confidence intervals. We assessed intervention compliance as odds ratios with corresponding 95% confidence intervals.
For studies involving two or more interventions classified as the same treatment node, with at least one other comparison intervention available (eg, a study involving three arms, in which two arms were classified as physiotherapy care, and the third arm was classified as pain education), data from the duplicated treatment nodes were pooled and the study was included in the meta-analyses. However, studies that compared only the same type of psychological intervention, without any other comparison interventions (eg, a study involving two arms, where both arms were classified as cognitive behavioural therapy), were excluded from the meta-analyses.
We classified magnitudes of effect according to the following criteria: small or slight (SMD ≥0.20 to <0.50), moderate (SMD ≥0.50 to <0.80), or large or substantial (SMD ≥0.80).4445 We also selected SMD values of 0.50 as the cut-off point for clinical effectiveness, which was equivalent to a mean difference of the following values between groups:
2.3 points on the Roland Morris Disability Questionnaire (0 to 24) scale for physical function (that is, 9.7 points difference on a 0 to 100 scale);
12.7 points on the Modified Von Korff (0 to 100) scale for pain intensity; and
3.3 points on a Fear Avoidance Beliefs Questionnaire (0 to 24) scale for fear avoidance (that is, 13.4 points difference on a 0 to 100 scale).
To transform SMD to mean difference values, based on a methodological paper,46 we multiplied the SMD by the pooled standard deviation obtained from the largest trial assessing each outcome: physical function,47 pain intensity,47 and fear avoidance.47 We used Stata (version 14) for all analyses.48 We used the metan command (with Hartung-Knapp-Sidik-Jonkman adjustment applied) for the pairwise meta-analyses, and the network package and network graphs package for the NMA.48
We attempted but were unable to perform a meta-analysis for health related quality of life and safety, owing to heterogeneity of assessment or reporting or both. The results of studies assessing health related quality of life were summarised descriptively. For safety, we dichotomised studies into two groups. The first consisted of studies that provided clear information about adverse effects occurring during the intervention period, including information about relatedness to the intervention or interventions under investigation (which were summarised descriptively). The second group included studies that did not provide clear information about any adverse effects occurring during the intervention period, including information about relatedness to the intervention or interventions under investigation. Only results of studies from the first group for safety were summarised descriptively.
Dealing with missing outcome data and missing statistics
For continuous outcomes, we imputed missing data by converting standard errors, P values, or confidence intervals into standard deviations.26 If a study reported only the median or interquartile range, the standard deviation was calculated by dividing the interquartile range by 1.35, and we considered the median to be equivalent to the mean. If relevant information was provided in figures, we extracted data from the graphs. Authors were contacted when data could not be obtained. We performed sensitivity analyses excluding data imputed from median and interquartile range values, which was only relevant to the primary outcomes, to examine the robustness of our primary analyses. Effect estimates were highly similar to our primary analysis in terms of the magnitude and certainty of the effect, and clinical significance (supplementary N).
Assumptions of transitivity and consistency
We assessed transitivity by visual inspection of a table containing categorised study characteristics: mode study setting (inpatient, outpatient, outpatient online only); intervention duration (weeks); mode of study-level mean participant age, dichotomised as younger than 50 years or 50 years and older; mode of study-level sex distribution, dichotomised as a population of less than 50% of male individuals or 50% or more of male individuals; and outcome scales reported. Global inconsistency of the entire network was assessed by the design-by-treatment interaction model.49 Local inconsistencies were assessed by the Bucher method.50 If global inconsistency was detected, we explored possible causes of inconsistency through sensitivity analyses.
Evaluation of small-study effects
Small-study effects were evaluated by visual inspection of comparison-adjusted funnel plots, including only comparisons with at least one study available, for asymmetry.49 We performed meta-regression using the total sample size to detect small-study effects.51 We attempted to perform a sensitivity analysis by excluding studies with a sample size of less than 100; however, this process resulted in the exclusion of 53 (55%) of 97 studies from our systematic review, leading to large changes in our network structure. Therefore, this additional analysis was not performed.
Sensitivity and subgroup analyses
To examine the robustness of our results and to examine sources of potential inconsistency, we performed the following sensitivity analyses at post-intervention: firstly, excluding studies with high risk of bias; secondly, including only studies using intention-to-treat analysis; thirdly, excluding studies published before the year 2000; and finally, excluding studies of patients with leg pain. To examine whether older studies resulted in remarkable changes in effect estimates, we also performed two additional sensitivity analyses for each of the primary outcomes, excluding studies published before year 1995 and before year 2005. For outcomes analysed quantitatively, we did meta-regression at each time point based on mean age, percentage of male individuals, and sample size.
For physical function, pain intensity, and fear avoidance, we performed meta-regression at each time point based on baseline values of the respective outcome. Because study authors used different measurement scales, we converted baseline data to standardised 0 to 100 (maximum) scales before performing meta-regressions. Subgroup analyses based on meta-regression results were only performed when both of the following criteria were met: P value of the regression coefficient was less than 0.05 and 10 or more studies were available for the relevant comparison.52 If inconsistency continued to persist in the network, we then sought to remove it by performing sensitivity analyses excluding portions of evidence in the network,49 based on visual inspection of possible sources of intransitivity across relevant studies. For these analyses, which were only relevant to the primary outcomes, we presented the justifications for exclusion, the resulting effect estimates, and the corresponding global tests of inconsistency (showing no detected inconsistency) in supplementary N. Owing to heterogeneity of reporting, we were unable to perform meta-regression based on intervention dosage or frequency. We attempted but were unable to perform subgroup analyses based on intervention delivery format (that is, face-to-face, telephone administered, web based, self-help booklets, and hybrid; dichotomised as face-to-face or other delivery format) or setting (that is, individual, group based, and hybrid; dichotomised as group based or other delivery setting). After dichotomising interventions according to delivery format and setting, we observed large changes in the network structure (that is, many treatment nodes became disconnected, resulting in networks that were dissimilar to the primary network plots). Therefore, we did not proceed with subgroup analyses.
Patient and public involvement
This study is an NMA of previously published studies. No patients were involved in setting the research question or the outcome measures, nor were they involved in developing plans for the design and conduct of the study. No patients were asked to advise on interpretation or writing up of results.
Results
Overall, 7983 records were identified from electronic database (6919 records) and registry searches (1064 records). After removing duplicates, 4728 records were screened for titles and abstracts, and 235 full text articles were screened for eligibility (see supplementary C). From electronic database and registry searching, we identified 70 eligible articles. An additional 27 records which were identified from other sources (that is, reference lists of relevant systematic reviews9101112131415 and clinical guidelines,172253 citation alerts, and contacting authors of included studies) were also included in the review. No cluster randomised controlled trials were eligible for inclusion in our review. In total, 97 articles involving 97 unique studies and 13 136 people with chronic, non-specific LBP were included in the systematic review (fig 1). Figure 2 and figure 3 depict the network plots for the primary outcomes (supplementary Q).
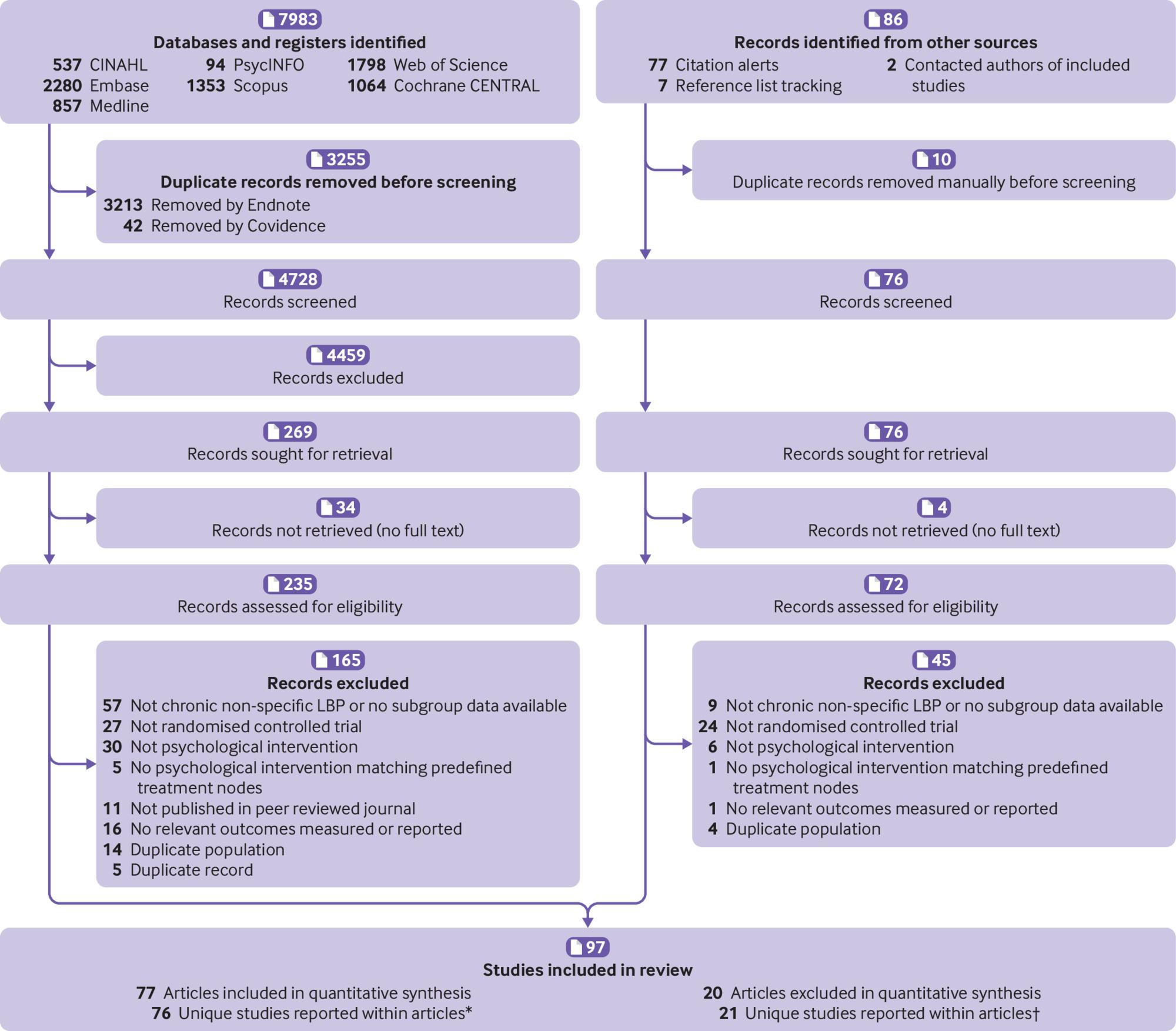
Study selection flowchart. *One article reported data on two unique studies, one article reported long term follow-up data, and one article provided additional baseline data that were not available in a related, included article reporting the same study. †One article reported long term follow-up data for two unique studies. LBP=lower back pain
{kind=link}

Network plots of physical function and pain intensity at post-intervention and short term follow-up. Adv=advice; BT=behavioural therapy; BT+PC=behavioural therapy delivered with physiotherapy care; CBT=cognitive behavioural therapy; CBT+PC=cognitive behavioural therapy delivered with physiotherapy care; CP=combined psychological approaches; CP+PC=combined psychological approaches delivered with physiotherapy care; Csl=counselling; Csl+PC=counselling delivered with physiotherapy care; GP=general practitioner care; Mind=mindfulness; Mind+PC=mindfulness delivered with physiotherapy care; NI=no intervention; PE=pain education; PE+PC=pain education delivered with physiotherapy care; PC=physiotherapy care; UC=usual care
{kind=link}

Network plots of physical function and pain intensity at mid-term and long term follow-up. Adv=advice; BT=behavioural therapy; BT+PC=behavioural therapy delivered with physiotherapy care; CBT=cognitive behavioural therapy; CBT+PC=cognitive behavioural therapy delivered with physiotherapy care; CP=combined psychological approaches; CP+PC=combined psychological approaches delivered with physiotherapy care; Csl=counselling; GP=general practitioner care; Mind=mindfulness; Mind+PC=mindfulness delivered with physiotherapy care; NI=no intervention; PC=physiotherapy care; PE=pain education; PE+PC=pain education delivered with physiotherapy care; UC=usual care
{kind=link}
Overview of studies
Table 2 presents general characteristics of the 97 included studies, separated by study outcomes (supplementary D and E). Post-intervention was the most frequently assessed time point across all outcomes. Most studies were published between 2011 and 2021 and were conducted in Europe (table 2). Physiotherapy care was the most frequently investigated comparison intervention for all outcomes. Mean body mass index and study sample size were similar across studies assessing physical function and pain intensity (table 2). However, mean age and percentage of males differed slightly across studies assessing physical function and pain intensity (table 2).
General characteristics of all included studies
Overall, the reporting of socioeconomic information (eg, occupational status, educational levels, income, race, or ethnic minority) was poor and inconsistent across the included studies. For example, 32 (33%) of 97 included studies reported information on occupational status, of which only 14 reported study level data. Of 97 included studies, 32 (33%) reported information on educational levels, of which only 10 studies reported study level data. To explore whether these factors were potential effect modifiers, we attempted but were unable to impute arm level data from the remaining studies, owing to heterogeneity of reporting by study authors, precluding subgroup analyses or meta-regression.
Twenty one unique studies were not included in the NMA for physical function and pain intensity, and eight unique studies were not included in the NMA for fear avoidance (see supplementary G).
Exploring potential heterogeneity of the physiotherapy care node
To explore potential heterogeneity in the physiotherapy care reference node, we summarised all studies that investigated physiotherapy care, delivered as a non-psychological co-intervention or comparison intervention (supplementary F). In total, 44 unique studies included at least one intervention arm of physiotherapy care as a non-psychological co-intervention. From these 44 studies, 36 (82%) investigated exercise alone, six (14%) investigated exercise with passive therapy, and two (5%) investigated passive therapy alone, as non-psychological co-interventions. In total, 33 unique studies included at least one intervention arm involving physiotherapy care as a comparison intervention. From these 33 studies, 19 (58%) investigated exercise alone, nine (27%) investigated exercise with passive therapy, and four (12%) investigated passive therapy alone, as comparison interventions. Additionally, one study (3%) had two comparison arms classified as physiotherapy care (one arm involving the combined delivery of exercise with passive therapy and the other arm involving passive therapy delivered alone), which were pooled in the NMA. Overall, the physiotherapy care node mainly consisted of exercise interventions only, followed by a smaller number of studies investigating exercise delivered with passive therapy. Passive therapy was infrequently delivered alone, either as a co-intervention or a comparison intervention. Therefore, despite potential limitations of combining interventions considered effective (that is, exercise), ineffective (that is, passive therapies alone), and possibly effective (that is, exercise delivered with passive therapy) for chronic LBP,17 we assumed that heterogeneity was unlikely to significantly affect the study results because most relevant studies involved exercise or exercise with passive therapy.
Transitivity
We summarised the study characteristics across direct comparisons within the network for physical function, pain intensity, fear avoidance, and intervention compliance (supplementary H). The mode study setting was balanced across all comparisons (conducted in outpatient settings) except in five (13%) of 38 comparisons for physical function, four (10%) of 40 comparisons for pain intensity, four (22%) of 18 comparisons for fear avoidance, and one (8%) of 13 comparisons for intervention compliance. Across dissimilar comparisons, online outpatient setting was the mode study setting across three (60%) of five comparisons for physical function, two (50%) of four comparisons for pain intensity, two (50%) of four comparisons for fear avoidance, and one (100%) of one comparisons for intervention compliance.
For physical function and pain intensity, the mode study level mean participant age appeared to be similar across most comparisons (<50 years), except in four (11%) of 38 comparisons for physical function, eight (20%) of 40 comparisons for pain intensity, four (22%) of 18 comparisons for fear avoidance, and three (23%) of 13 comparisons for intervention compliance. On further inspection, the mean age in four (67%) of six individual studies comprising the dissimilar comparisons for physical function was younger than 51.6 years,54555657 and the mean age in nine (64%) of 14 studies comprising the dissimilar comparisons for pain intensity was younger than 53.4 years.545556585960616263 The mean age was younger than 53.3 years in four (67%) of six individual studies comprising dissimilar comparisons for fear avoidance,55565964 and three (60%) of five studies comprising the dissimilar comparisons for intervention compliance.555960
Although mode study level distribution of sex was similar across most comparisons for the primary outcomes (<50% males), 10 (26%) of 38 comparisons for physical function and 14 (35%) of 40 comparisons for pain intensity either had a mode of 50% or more males, or a bimodal distribution of sex. However, for physical function, the distribution of sex in six (67%) of nine unique studies comprising the dissimilar comparisons was less than 55% males,656667686970 while for pain intensity, the distribution of sex in 10 (59%) of 17 unique studies comprising the dissimilar comparisons was less than 54% males.60656668707172737475 For the secondary outcomes, the mode study-level distribution of sex was similar across most comparisons except in three (17%) of 18 comparisons for fear avoidance and four (31%) of 13 comparisons for intervention compliance. For fear avoidance, the distribution of sex in three (50%) of six individual studies comprising the three dissimilar comparisons was less than 52% males.646569 For intervention compliance, the distribution of sex in two (33%) of six individual studies comprising the four dissimilar comparisons was less than 58% males,6076 while the distribution of sex in the remaining studies ranged from 62% to 88% males.597778 Nonetheless, meta-regression did not suggest that either mean age or proportion of males were effect modifiers (supplementary Y).
In addition, meta-regression based on mean baseline levels of physical function, pain intensity, or fear avoidance did not suggest these factors were effect modifiers (supplementary Y). The duration of intervention was also similar, mostly between two weeks and 12 weeks in length, across different comparisons involving the same types of psychological interventions. Overall, we considered the assumption of transitivity was valid.
Risk of bias within included studies
The domain level and overall risk of bias judgments for physical function, pain intensity, and fear avoidance are presented in supplementary J. A risk-of-bias assessment was not applicable to intervention compliance. For physical function, of 61 unique studies included in the NMA, 58 were judged as having some concerns and three were judged as having high risk of bias. For pain intensity, of 66 unique studies, 62 were judged as having some concerns and four were judged as having high risk of bias. For fear avoidance, of 30 unique studies included, 29 studies were judged as having some concerns and one study was judged as having high risk of bias. For all relevant outcomes, the main concerns related to risk of bias were pertaining to measurement of the outcome (domain four) and selection of the reported result (domain five). Sensitivity analyses excluding studies with high risk of bias did not substantially affect the results of the global or local inconsistency tests, suggesting studies with high risk of bias were not an important source of inconsistency.
Psychological interventions for physical function
Of 80 articles assessing physical function, 62 articles that reported data for 61 unique studies and involved 9397 people with chronic, non-specific LBP, were included in the NMA. The median time point for assessment for post-intervention was at the end of treatment (range 0-2 months post-intervention). The other median follow-up time points were 3 months (2-5 months) post-intervention for short term follow-up, 9 months (6-11 months) post-intervention for mid-term follow-up, and 12 months (12-33 months) post-intervention for long term follow-up. Physical function was assessed with the Oswestry Disability Index (English and Italian versions), Roland Morris Disability Questionnaire (23 item, 18 item, 16 item, and Spanish versions), Quebec Back Pain Disability Scale (English and Portuguese versions), Low Back Outcome Scale, modified Von Korff Scale, Hannover Activities of Daily Living Questionnaire, Activities of Daily Living Questionnaire, and Pain Disability Index and Pain and Disability Index (Million). Results of the NMA and CINeMA assessment (domain level judgments and overall confidence ratings) for physical function are presented in supplementary I and K.
We did not detect any inconsistency at post-intervention or long term follow-up for physical function (supplementary O). However, we detected global inconsistency at short term and mid-term follow-up (supplementary O). At these time points, local inconsistency was detected in four (22%) of 18 pairwise comparisons at short term follow-up, and five (24%) of 21 pairwise comparisons at mid-term follow-up (supplementary P). Sensitivity analyses were conducted at short term and mid-term follow-up for physical function, which resolved the presence of inconsistency at these time points. We resolved inconsistency at short term follow-up by removing three studies contributing to intransience related to the measurement tools for assessing physical function, for pairwise comparisons showing inconsistency.68798081 Inconsistency at mid-term follow-up was resolved by removal of the same three studies contributing to intransience related to the measurement tools for assessing physical function at short term follow-up.68798081 Additionally, one study contributing direct evidence to the pairwise comparison between cognitive behavioural therapy delivered with physiotherapy care and physiotherapy care alone, which showed inconsistency, and was removed (supplementary N).82
The NMA results showed that at post-intervention, cognitive behavioural therapy delivered with physiotherapy care (SMD 1.01, 95% confidence interval 0.58 to 1.44; moderate quality evidence; equivalent to 19.6 points mean difference in improvement on a scale of 0 to 100), and pain education delivered with physiotherapy care (0.62, 0.08 to 1.17; moderate quality evidence; equivalent to 12.0 points mean difference in improvement on a scale of 0 to 100) had large and moderate clinically important effects, respectively, for improving physical function in comparison with physiotherapy care alone (fig 4). Sensitivity analysis excluding two studies with high risk of bias produced similar effect estimates (1.09, 0.62 to 1.57 for cognitive behavioural therapy with physiotherapy care; and 0.63, 0.07 to 1.20 for pain education with physiotherapy care; supplementary N). Results from all other sensitivity analyses conducted for physical function at post-intervention were similar to those of the primary analysis (supplementary N).

Forest plot of network meta-analysis results for physical function at post-intervention. *Denotes significance at p<0.05. BT=behavioural therapy; CBT=cognitive behavioural therapy; Comb psych=combined psychological approaches; Csl=counselling; GP care=general practitioner care; PE=pain education; SMD=standardised mean difference. Physiotherapy care was the reference comparison group
{kind=link}
From the primary analysis, the effects of cognitive behavioural therapy delivered with physiotherapy care were maintained at short term follow-up (SMD 0.60, 95% confidence interval 0.20 to 1.00; moderate quality evidence; moderate and clinically important effect), and at mid-term follow-up (0.34, 0.13 to 0.56; moderate quality evidence; small and not clinically important effect). In contrast, results from the sensitivity analyses (resolving inconsistency) found that at short term follow-up, the effect of treatment was small and not clinically important (0.31, 0.01 to 0.61); results at mid-term follow-up were similar to effect estimates obtained in the primary analysis (0.25, 0.09 to 0.41; supplementary N). At long term follow-up, cognitive behavioural therapy delivered with physiotherapy care was not statistically significant compared with physiotherapy care alone (1.56, −0.10 to 3.21, supplementary I).
The primary analysis showed that compared with physiotherapy care alone, pain education delivered with physiotherapy care maintained a moderate and clinically significant effect at short term follow-up (SMD 0.63, 95% confidence interval 0.25 to 1.00; low quality evidence). Sensitivity analysis (resolving inconsistency) indicated that the effects of treatment were large and clinically important (0.85, 0.56 to 1.15; equivalent to 16.5 points mean difference in improvement on a scale of 0 to 100; low to moderate quality evidence). Nonetheless, at mid-term follow-up, results from both the primary analysis (0.67, −0.03 to 1.37; low quality evidence) and sensitivity analysis (resolving inconsistency) (0.39, −0.17 to 0.95; low quality evidence) found that treatment effects were no longer significant. No studies investigated the effect of pain education delivered with physiotherapy care in the long term.
Compared with physiotherapy care, only small or no treatment effects on physical function were observed for other types of psychological interventions, delivered with or without physiotherapy care, at post-intervention or follow-up time points (supplementary I and supplementary N).
Based on the SUCRA values and mean rank (supplementary L), the most highly ranked intervention at post-intervention was cognitive behavioural therapy delivered with physiotherapy care (SUCRA 92.3% and mean rank 2.2). At short term and mid-term follow-up, pain education delivered with physiotherapy care ranked first (for short term, 85.6% and 2.7; for mid-term, 90.7% and 2.3). At long term follow-up, cognitive behavioural therapy delivered with physiotherapy care ranked first (62.7% and 4.4). Rankograms for physical function are presented in supplementary L. In the sensitivity analysis (resolving inconsistency) at short term follow-up, pain education delivered with physiotherapy care remained the most highly ranked intervention (SUCRA 99.9%). In the sensitivity analysis (resolving inconsistency) at mid-term follow-up, combined psychological approaches delivered with physiotherapy care was ranked first (94.6%), followed by pain education delivered with physiotherapy care (84.5%). The comparison-adjusted funnel plots (supplementary M), and meta-regression based on sample size (supplementary Y), did not suggest small-study effects for physical function at any time points. We did not find any evidence suggesting that mean age, proportion of males, or mean baseline levels of physical function were effect modifiers (supplementary Y).
Psychological interventions for pain intensity
Of 86 articles assessing pain intensity, 67 articles reported data for 66 unique studies and involved 9462 people with chronic, non-specific LBP and were included in the NMA. For post-intervention, the median time point for assessment was at the end of treatment (range 0-2 months post-intervention). Median follow-up time points were 3 months (range 2-5 months), 9 months (6-11 months), and 12 months (12-60 months) post-intervention for short term, mid-term, and long term follow-up, respectively. Pain intensity was assessed with the Numeric Rating Scale (using scale ranges of 0-100, 0-10, and 0-20), Visual Analogue Scale (100 mm and 10 mm versions), bodily pain subscale of the SF-36, Pain Rating Chart, pain intensity subscale of the Low Back Outcome Score, Brief Pain Inventory, Box Scale, Pain Intensity Questionnaire, modified Von Korff pain scale, McGill Pain Questionnaire (short form version and Pain Rating Index subscale; English and Turkish versions), Graded Chronic Pain Scale, Chronic Pain Grade Questionnaire, Functional Rating Index Test, and Descriptor Differential Scale. We present the results of the NMA and CINeMA assessment (domain level judgments and overall confidence ratings) for pain intensity in supplementary I and K. We did not detect global inconsistency at post-intervention, mid-term, or long term follow-up for pain intensity (supplementary O). However, global inconsistency was detected at short term follow-up (supplementary O), with five (20%) of 25 pairwise comparisons indicating local inconsistency at this time point (supplementary P). Inconsistency for pain intensity at short term follow-up was resolved by removing one study that contributed to intransience related to intervention duration,83 and one study that contributed direct evidence to all pairwise comparisons showing inconsistency (supplementary N).84
The NMA results showed that at post-intervention, behavioural therapy delivered with physiotherapy care (SMD 1.08, 95% confidence interval 0.22 to 1.94; low quality evidence; equivalent to 27.3 points mean difference in improvement on a scale of 0 to 100), cognitive behavioural therapy delivered with physiotherapy care (0.92, 0.43 to 1.42; moderate quality evidence), and pain education delivered with physiotherapy care (0.91, 0.37 to 1.45; moderate quality evidence) have a large and clinically important effect on reducing pain intensity, compared with physiotherapy care alone (supplementary I; fig 5). Sensitivity analysis, excluding three studies with high risk of bias, produced similar effect estimates (1.14, 0.04 to 2.24 for behavioural therapy with physiotherapy care; 0.91, 0.37 to 1.46 for cognitive behavioural therapy with physiotherapy care; and 0.91, 0.35 to 1.48 for pain education with physiotherapy care; supplementary N). Results from all other sensitivity analyses conducted for pain intensity at post-intervention were similar, except for cognitive behavioural therapy delivered with physiotherapy care, which was not significant in the sensitivity analysis excluding studies of patients with leg pain (0.56, −0.01 to 1.12; supplementary N).
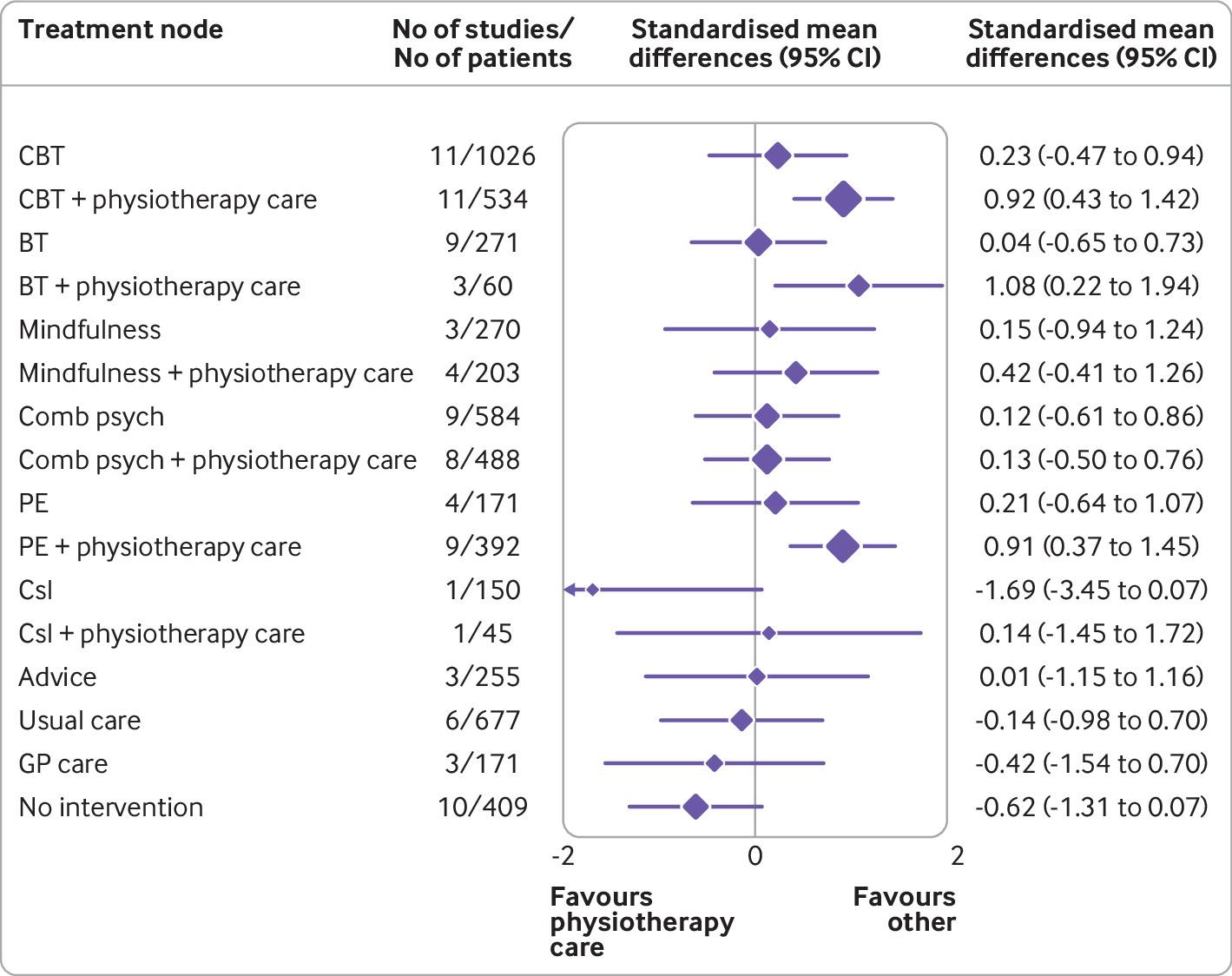
Forest plot of network meta-analysis results for pain intensity at post-intervention. *Denotes significance at p<0.05. BT=behavioural therapy; CBT=cognitive behavioural therapy; Comb psych=combined psychological approaches; Csl=counselling; GP care=general practitioner care; PE=pain education. SMD=standardised mean difference. Physiotherapy care was the reference comparison group
{kind=link}
From the primary analysis, behavioural therapy delivered with physiotherapy care maintained a large and clinically important effect on reducing pain intensity at short term follow-up (SMD 2.15, 95% confidence interval 0.27 to 4.03; moderate quality evidence). However, when we performed sensitivity analysis to resolve inconsistency at this time point, behavioural therapy delivered with physiotherapy care became disconnected from the network, precluding our ability to examine the robustness of these findings at short term follow-up (supplementary N). Nonetheless, we did not detect inconsistency at mid-term follow-up, and our results showed that behavioural therapy delivered with physiotherapy had a large and clinically important effect for reducing pain intensity, compared with physiotherapy care (1.01, 0.41 to 1.60; high quality evidence; equivalent to 25.6 points mean difference in improvement on a scale of 0 to 100). Effect estimates at long term follow-up suggested a large effect of treatment; however, the results were not significant (0.86, −1.12 to 2.84; moderate quality evidence).
The primary analysis showed that compared with physiotherapy care, cognitive behavioural therapy delivered with physiotherapy care was not significant for reducing pain intensity at short term follow-up (SMD 0.47, 95% confidence interval −0.66 to 1.61; moderate quality evidence). However, after sensitivity analysis (resolving inconsistency), we identified a moderate and clinically important effect at this time point (0.67, 0.01 to 1.33; moderate quality evidence; supplementary N). Nonetheless, significance was attenuated at mid-term (0.28, −0.01 to 0.57; moderate quality evidence) and long term follow-up (1.19, −0.10 to 2.48; moderate quality evidence).
Both the primary analysis (SMD 1.04, 95% confidence interval 0.19 to 1.88; moderate quality evidence; supplementary I) and sensitivity analysis (1.06, 0.56 to 1.55; supplementary N) found that pain education delivered with physiotherapy care maintained a large and clinically important effect at short term follow-up. The effect of treatment remained significant at mid-term follow-up, although the effect was small and not clinically important (0.41, 0.13 to 0.95; moderate quality evidence). No studies investigated the effect of pain education delivered with physiotherapy care on pain intensity in the long term.
We noted a large and clinically important difference between no intervention and physiotherapy care alone in reducing pain intensity at short term follow-up, favouring physiotherapy care (SMD −2.06, 95% confidence interval −3.51 to −0.60; moderate quality evidence). However, the effect did not remain after the sensitivity analysis (resolving inconsistency) (0.21, −0.86 to 1.28; supplementary N). The only other psychological intervention that had a significant effect on reducing pain intensity, compared with physiotherapy care, was pain education at mid-term follow-up (0.75, 0.16 to 1.35; low quality evidence).
Based on the SUCRA values and mean rank (supplementary L), the most highly ranked intervention at post-intervention (SUCRA 91.2%, mean rank 2.4), short term (96.7%, 1.4), and mid-term (96.6%, 1.5) follow-up was behavioural therapy delivered with physiotherapy care. At long term follow-up, cognitive behavioural therapy delivered with physiotherapy care was the highest ranked intervention (69.2%, 3.8). Rankograms for pain intensity are presented in supplementary L. In sensitivity analysis (removing inconsistency) at short term follow-up, behavioural therapy delivered with physiotherapy care became disconnected from the network, therefore, no SUCRA results were available. Instead, pain education delivered with physiotherapy care was the most highly ranked intervention (SUCRA 92.3%) at this time point. The comparison-adjusted funnel plots (supplementary M), and meta-regression based on sample size (supplementary Y), did not suggest small-study effects for pain intensity at any time points. We did not find any evidence suggesting that mean age, percentage of males, or mean baseline levels of pain intensity were effect modifiers (supplementary Y).
Psychological interventions for fear avoidance
Of 37 articles assessing fear avoidance, 29 articles that reported data for 29 unique studies and involved 4288 people with chronic, non-specific LBP, were included in the NMA. The network became disconnected at long term follow-up. For post-intervention, the median time point for assessment was at the end of treatment (range 0-2 months post-intervention). The median follow-up time points were 3 months (range 2-5 months) and 9 months (6-11 months) post-intervention for short term and mid-term follow-up, respectively. Fear avoidance was assessed using the Fear Avoidance Beliefs Questionnaire, Pain Catastrophising Scale, Tampa Scale of Kinesiophobia (English, Italian, Portuguese, and shortened versions), Pain Coping and Cognition List (Catastrophising subscale), and Coping Strategies Questionnaire (Catastrophising scale). Results of the NMA, risk-of-bias assessment for each study (domain level judgments and overall risk of bias), and CINeMA assessment (domain level judgments and overall confidence rating) for fear avoidance are presented in supplementary Q and R. We did not detect any global or local inconsistency for fear avoidance at any time (supplementary W and X). We did not find any evidence suggesting that mean age, proportion of males, or mean baseline levels of fear avoidance were effect modifiers.
The NMA results showed that at post-intervention, cognitive behavioural therapy delivered with physiotherapy care had a large and clinically important effect on reducing fear avoidance, compared with physiotherapy care alone (SMD 1.77, 95% confidence interval 0.65 to 2.90; moderate quality evidence; equivalent to 47.4 points mean difference in improvement on a scale of 0 to 100). No other psychological interventions showed any significant differences compared with physiotherapy care alone. Sensitivity analysis excluding one study with high risk of bias resulted in similar effect estimates (1.79, 0.58 to 2.99; supplementary V). However, significance and clinical effectiveness were attenuated in the results from the sensitivity analysis that excluded studies of patients with leg pain (0.39, −0.04 to 0.82). In contrast, pain education delivered either alone (0.92, 0.25 to 1.60) or with physiotherapy care (1.03, 0.61 to 1.45) showed a large and clinically important effect on reducing fear avoidance (supplementary V).
At short term (SMD 0.01, 95% confidence interval −0.73 to 0.74; moderate quality evidence) and mid-term follow-up (0.50, −0.08 to 1.07; low quality evidence), cognitive behavioural therapy delivered with physiotherapy care had no significant effect on reducing fear avoidance, compared with physiotherapy care. Owing to disconnection of the network at long term follow-up, we performed only a pairwise meta-analysis of cognitive behavioural therapy delivered with physiotherapy care and physiotherapy care alone. The results were not significant; however, the 95% confidence interval suggested that results might favour cognitive behavioural therapy delivered with physiotherapy care (3.21, 0.00 to 6.41).
In contrast, pain education delivered alone (SMD 1.34, 95% confidence interval 0.38 to 2.30; moderate quality evidence) or with physiotherapy care (0.92, 0.50to 1.34; moderate quality evidence) had large and clinically important effects on reducing fear avoidance at short term follow-up. However, based on low quality evidence, treatment effects did not remain at mid-term follow-up (0.76, -0.11 to 1.62 for pain education delivered alone; 0.41, -0.36 to 1.19 for pain education delivered with physiotherapy care), with no network evidence available at long term follow-up.
The only other psychological intervention to show any significant effects on reducing fear avoidance, compared with physiotherapy care, was combined psychological approaches alone. The effects of treatment were observed only at short term follow-up (SMD 1.70, 95% confidence interval 0.38 to 3.02; moderate quality evidence), with no network evidence available at long term follow-up.
Based on the SUCRA values and mean rank (supplementary S), the most highly ranked intervention at post-intervention was cognitive behavioural therapy delivered with physiotherapy care (SUCRA 71.3%, mean rank 4.2). At short term follow-up, combined psychological approaches was ranked first (90.4%, 1.7), whereas pain education alone was ranked first at mid-term follow-up (80.5%, 3.3). SUCRA and mean rank were not assessed at long term follow-up because the network became disconnected. The comparison-adjusted funnel plots (supplementary T) and meta-regression based on sample size (supplementary Y) did not indicate small-study effects for fear avoidance at any time points. We did not find any evidence suggesting that mean age, percentage of males, or mean baseline levels of fear avoidance were effect modifiers (supplementary Y).
Psychological interventions for intervention compliance
Of 38 articles reporting enough data to assess intervention compliance, we included 25 articles that reported data for 26 unique studies and involved 2877 people with chronic, non-specific LBP in the NMA done at post-intervention (supplementary Q). We did not detect any global or local inconsistency for intervention compliance (supplementary W and X).
Compared with physiotherapy care, only combined psychological approaches significantly increased the odds of intervention compliance (odds ratio 0.28, 95% confidence interval 0.09 to 0.86; moderate quality evidence). The sensitivity analysis that excluded one study with high risk of bias produced similar effect estimates for combined psychological approaches (0.30, 0.10 to 0.94; supplementary V). However, significance was lost for combined psychological approaches, compared with physiotherapy care, in all other sensitivity analyses (supplementary V). No interventions showed a significant effect on reducing the odds of intervention compliance, compared with physiotherapy care, in the primary or sensitivity analyses.
Based on the SUCRA values and mean rank (supplementary S), the most highly ranked intervention for improving intervention compliance was combined psychological approaches (SUCRA 78.7%, mean rank 2.9). The comparison-adjusted funnel plots (supplementary T) and meta-regression based on sample size did not indicate small-study effects for intervention compliance at post-intervention. We did not find any evidence suggesting that mean age or percentage of males were effect modifiers (supplementary Y).
Psychological interventions for health related quality of life
Of 44 unique studies assessing health related quality of life, 18 studies involving 2079 people with chronic, non-specific LBP involved a physiotherapy care comparison group (supplementary U). In these studies, health related quality of life was assessed using the SF-12 (physical component summary score), SF-36 (physical component summary score, overall score, individual scores of all or some subscales), Sickness Impact Profile, Quality of Life Scale, and a question initiated by investigators about the overall assessment of quality of life.
The available evidence suggests that pain education delivered alone6870 or in conjunction with physiotherapy care,8586 cognitive behavioural therapy delivered with physiotherapy care,8788 and counselling delivered with physiotherapy care89 are more effective than physiotherapy care alone for improving health related quality of life. Evidence is conflicting for the effectiveness of combined psychological approaches delivered with physiotherapy care for improving health related quality of life, compared with physiotherapy care alone (ranging from no effect90 to a significant effect at short term91 or long term follow-up9293). Similarly, evidence is mixed regarding the effect of mindfulness delivered with physiotherapy care on health related quality of life, compared with physiotherapy care (no effect6263 to short term effects only6194). Behavioural therapy, delivered alone or in conjunction with physiotherapy care, did not appear to be more effective than physiotherapy care alone for improving health related quality of life.727484
Safety of different types of psychological interventions
In total, 20 unique studies provided enough information about the number and relatedness of adverse effects occurring during the intervention period. Of these studies, 12 (60%) clearly reported that no adverse events occurred in any intervention group.556776828589909596979899 One study comparing cognitive behavioural therapy with no intervention reported that no serious adverse effects (defined as death or admission to hospital, events attributable to the intervention, or events that caused unwarranted distress to a participant) occurred in either group, during the intervention period.47 Four studies reported on the occurrence of adverse events during the intervention period5461100101; however, none was related to the psychological interventions under investigation. Three studies reported that adverse effects occurred in the psychological intervention group.626669 The adverse effects included: increased back pain (three (5%) of 61 participants allocated to cognitive behavioural therapy delivered with physiotherapy care)66; worsening of symptoms during treatment (one (2%) of 43 participants allocated to behavioural therapy alone)69; and emergence of painful emotional memories (one (6%) of 16 participants allocated to mindfulness delivered with physiotherapy care).62 No event was considered as a serious adverse effect by the study authors.
Discussion
Principal findings
Compared with physiotherapy care alone (mainly structured exercise), physiotherapy delivered with psychological interventions are more effective for improving physical function and pain intensity in people with chronic, non-specific LBP. Based on moderate quality evidence, cognitive behavioural therapy delivered with physiotherapy care was the most effective intervention for improving physical function at post-intervention, compared with physiotherapy care (equivalent to 19.6 points mean difference in improvement on a scale of 0 to 100. However, the clinical effectiveness of treatment diminished at short term follow-up. In contrast, pain education delivered with physiotherapy care resulted in moderate effects at post-intervention (equivalent to 12.0 points mean difference in improvement on a scale of 0 to 100); although, the clinical benefits of treatment were more sustainable, at least until short term follow-up (equivalent of to 16.5 points mean difference in improvement on a scale of 0 to 100; low to moderate quality evidence).
Based on low to high quality evidence, behavioural therapy delivered with physiotherapy care was the most effective psychological intervention for reducing pain intensity at post-intervention, compared with physiotherapy care (equivalent to 27.3 points mean difference in improvement on a scale of 0 to 100). The clinically important effects of treatment were sustained at least until mid-term follow-up (equivalent to 25.6 points mean difference in improvement on a scale of 0 to 100). However, we emphasise caution with interpreting results at short term follow-up for behavioural therapy delivered with physiotherapy care because of the presence of inconsistency.
Based on moderate quality evidence, cognitive behavioural therapy delivered with physiotherapy was the most effective intervention for reducing fear avoidance at post-intervention (equivalent to a mean difference of 47.4 points mean difference in improvement on a scale of 0 to 100). Current evidence suggests that the effects of cognitive behavioural therapy delivered with physiotherapy can be sustained until mid-term and long term follow-up (low to moderate quality evidence). However, in people with chronic, non-specific LBP who do not report no concurrent leg pain, at short term follow-up, pain education delivered alone or with physiotherapy care is the most effective intervention for reducing fear avoidance (moderate quality evidence).
Our systematic review identified that combined psychological approaches resulted in greater odds of intervention compliance, compared with physiotherapy care alone, although these findings should be interpreted with some caution. We were unable to determine the comparative effectiveness of psychological intervention for improving health related quality of life owing to heterogeneity of reporting across included studies. However, current evidence suggests that pain education, cognitive behavioural therapy, or counselling, delivered with physiotherapy care, can be more effective than physiotherapy care alone for improving health related quality of life.
Overall, our review has identified that pain education, behavioural therapy, and cognitive behavioural therapy are the most effective psychological interventions for people with chronic, non-specific LBP at post-intervention, when delivered with physiotherapy care. The most sustainable effects of treatment for physical function and fear avoidance are achieved with pain education programmes, and for pain intensity they are achieved with behavioural therapy. Although their clinical effectiveness diminishes over time, particularly in the long term (≥12 months post-intervention), evidence supports the clinical benefits of combining physiotherapy care with these specific types of psychological interventions at the onset of treatment. The small total sample size at long term follow-up (eg, for physical function, n=6986 at post-intervention v n=2469 for long term follow-up; for pain intensity, n=6963 v n=2272) have resulted in wide confidence intervals at this time point; however, the magnitude and direction of the pooled effects seemed to consistently favour the psychological interventions delivered with physiotherapy care, compared with physiotherapy care alone. Future studies with longer follow-up periods are needed to further examine the long term effect of psychological interventions for people with chronic, non-specific LBP. Nonetheless, the limited but consistent available data suggest that psychological interventions are likely to be safe for people with chronic, non-specific LBP. Therefore, clinicians should consider incorporating psychological interventions with physiotherapy care (mainly structured exercise) to maximise improvements in health outcomes.
Strengths and limitations of this study
Our review had several strengths. Firstly, we used an NMA design to synthesise direct and indirect evidence on a wide range of psychological interventions available for managing chronic, non-specific LBP. This synthesis allowed us to simultaneously compare and rank many competing interventions within one coherent treatment network to determine the comparative effectiveness of psychological interventions for improving various outcomes important to patients with LBP. Importantly, we used a meticulous method to classify the psychological interventions, which has been described in the protocol paper25 and in supplementary B. In summary, we used the splitting approach proposed by Caldwell et al102 to separate different types of psychological interventions into distinct categories, and further, we delineated between psychological interventions delivered with or without co-interventions. This method is an important strength of our study because previous reviews have commonly grouped different types of psychological interventions together or grouped psychological interventions with or without co-interventions together, in a single comparison, potentially leading to heterogenous comparisons and inaccurate treatment effect estimates.
Further, we used a careful selection of search terms, extracted from many existing studies of psychological interventions for chronic pain conditions, to capture a broad range of psychological interventions. Importantly, we assessed core clinical outcomes for evaluating the efficacy or effectiveness of health interventions in people with non-specific LBP (eg, physical function, pain intensity, and health related quality of life).103 These clinical outcomes are also consistent with the consensus based treatment targets of exercise for people with chronic, non-specific LBP: to improve function, improve quality of life, reduce pain, meet patient specific goals, and reduce fear of movement.104 By investigating outcomes that are meaningful to patients and clinicians, our findings can help to support decision making about the use of psychological interventions for this population. In addition, we investigated the comparative safety of psychological interventions for chronic, non-specific LBP, which to our knowledge, has not been assessed comprehensively in previous reviews and is an important consideration when evaluating the risk-benefit ratio of health interventions.
This systematic review also had some limitations. Although we separated different types of psychological interventions into five broad but distinct categories to minimise heterogeneity, we made a pragmatic decision to combine interventions involving two or more types of psychological approaches into one treatment node. This decision could have resulted in heterogeneity of combinations of psychological interventions included within this treatment node. However, this pragmatic decision allowed us to gain enough statistical power and provide a simpler framework from which our findings could be translated more easily into clinical practice. Furthermore, our search strategy aimed to include the most common psychological interventions for patients with chronic, non-specific LBP. However, we identified one type of psychological intervention (hypnosis) that matched our inclusion criteria but did not match our predefined decision set for treatment nodes.105 Consensus within the review team resulted in the inclusion of the study in our review, but exclusion from the NMA because of an inadequate number of studies available for pooling.
We also acknowledge that inconsistency was detected at various time points of analysis for our primary outcomes. If unresolved, the presence of inconsistency can threaten the validity of the NMA results. However, we performed a thorough examination of potential sources within the network (eg, visually inspecting study and patient characteristics to assess transitivity, exploring potential heterogeneity within the physiotherapy care node, and conducting numerous sensitivity analyses and meta-regressions), and we were able to sufficiently identify and resolve the main sources of inconsistency. Interpretation of study findings were made with consideration of the results of both the primary and sensitivity analyses.
The poor and inconsistent reporting of patient involvement in the design or development of the interventions described in the included studies limited our ability to ascertain whether the psychological interventions are considered acceptable to patients in clinical practice. In parallel, the absence of patient advocates involved in the planning and interpretation of the analyses could be considered a limitation of this review. The inherent inability to blind participants in clinical trials involving psychological interventions should also be considered as a potential source of bias (eg, study results could favour psychological interventions, delivered with or without physiotherapy care, over comparison interventions such as usual care, no interventions, or even physiotherapy care alone). In addition, poor and inconsistent reporting of data for socioeconomic factors and comorbidities precluded examination of these factors as potential effect modifiers. Furthermore, although the decision to combine exercise, passive therapy, and physiotherapy into one node was pragmatic (that is, reflecting clinical practice), heterogeneity within the node was a potential limitation. However, we concluded that this potential heterogeneity was unlikely to significantly affect study results because most affected studies involved exercise only (36 (82%) of 44 studies with physiotherapy care as a co-intervention and 19 (58%) of 33 with physiotherapy care as a comparison intervention), or exercise delivered with passive therapy (six (14%) of 44 studies and nine (27%) of 33 studies, respectively).
Comparison with other studies
No previous studies have used NMA to synthesise evidence on psychological interventions for chronic, non-specific LBP. Although several non-Cochrane systematic and narrative reviews have explored this topic, with and without pairwise meta-analysis, many have included non-randomised trials (eg, pilot or feasibility studies), which are prone to bias. Therefore, we compared our findings with the most recent Cochrane review of behavioural interventions for chronic LBP conducted by Henschke et al in 2010,14 which was an update of the Cochrane review conducted by van Tulder et al in 2000.9
The Cochrane review by Henschke et al14 included 30 randomised controlled trials and evaluated three types of behavioural therapies for chronic LBP: operant, cognitive, and respondent therapies. The review found that behavioural therapy delivered with physiotherapy and back education was not more effective than was physiotherapy care and back education alone for pain relief and physical function over the short to intermediate term. The review also found low to moderate quality evidence that behavioural therapy and group exercise did not differ significantly in reducing pain intensity. However, several methodological differences between our reviews made comparisons of findings difficult. Firstly, Henschke et al14 grouped psychological interventions, delivered alone or with non-psychological co-interventions, together within one comparison. For example, Henschke et al14 combined studies of cognitive behavioural therapy alone with studies of cognitive behavioural therapy with a structured exercise programme or as part of a multidisciplinary rehabilitation programme.14 In contrast, we delineated between cognitive behavioural therapy alone, and cognitive behavioural therapy with physiotherapy care co-interventions (mainly structured exercise), given that physiotherapy care and psychological interventions are traditionally delivered by distinct professions with different registration and training requirements. These professions are also governed by different hierarchical and interprofessional relationships. We sought to evaluate whether integration of these distinct therapies together, compared with delivery of these therapies in isolation, would result in differences in effect estimates.
Secondly, Henschke et al14 performed separate pairwise meta-analyses of behavioural therapies, cognitive therapy, and cognitive behavioural therapy, compared with waiting list controls. However, these authors also grouped behavioural therapies (that is, operant and respondent therapy) together with cognitive behavioural therapy into one comparison (called behavioural treatment) in separate meta-analyses comparing psychological interventions with either usual care, group exercise, or physiotherapy care.14 This grouping precluded examination of the differences between behavioural therapies and cognitive behavioural therapies, compared with exercise or physiotherapy care. In our review, we considered the distinction between behavioural therapy and interventions based on cognitive behavioural therapy to be important in our review, because we aimed to contrast traditional behavioural approaches (eg, biofeedback and progressive muscle relaxation) against contemporary behavioural approaches (eg, cognitive behavioural therapy), when compared with physiotherapy care. Furthermore, the clinical goal of physiotherapy care is typically grounded in changing behaviour, mainly through the promotion of exercise or physical activity. Although physiotherapists have been shown to partially recognise the presence of cognitive, psychological, and social factors in people with LBP, many do not have the confidence to deal with them.106 By delineating between behavioural therapy and interventions based on cognitive behavioural therapy, we sought to provide clinicians with important insights regarding the additional benefit of incorporating cognitive strategies into treatment, to maximise health outcomes for patients with chronic LBP.
Methodological differences probably reflect the paucity of studies available at the time of publication (that is, year 2010) for Henschke et al’s review.14 As reported in table 2, most studies included in our review were published between 2011 and 2021. Fear avoidance, health related quality of life, intervention compliance, and safety were not analysed statistically in the previous Cochrane review.14 We are not aware of any published high quality reviews directly comparing physiotherapy care with interventions based on pain education or counselling (that is, health coaching), delivered with or without a co-intervention, for people with chronic, non-specific LBP.
Implications for practice
Chronic pain conditions such as LBP require multimodal treatment approaches that address biopsychosocial dimensions.8 Our study fills an important gap in research by use of an NMA design to determine the comparative effectiveness, relative rankings, and safety of a wide collection of psychological interventions available for managing chronic, non-specific LBP. Firstly, our review has identified the specific types of psychological interventions that are most effective for physical function, pain intensity, and fear avoidance, in people with chronic, non-specific LBP, when combined with physiotherapy care (mainly structured exercise). We have also identified the specific types of psychological interventions that show no significant effect for these outcomes. We have shown that different types of psychological interventions are not equal in treatment effectiveness, and that the effect of treatment can differ between psychological interventions delivered alone compared with psychological interventions delivered with co-interventions (that is, mainly structured exercise). Importantly, we investigated the comparative safety of psychological interventions for this population to facilitate improved evaluation of the risk-benefit ratio of psychological interventions for chronic, non-specific LBP. Crucially, we also evaluated the comparative sustainability of treatment effectiveness for different psychological interventions. Findings from our study can be used to inform clearer guideline recommendations regarding the use of specific psychological interventions for managing chronic, non-specific LBP and support decision making for patients and clinicians.
For adults with chronic, non-specific LBP
Existing guidelines consistently endorse that exercise and psychosocial therapies should be prescribed for management of chronic LBP.16 However, guidelines are vague regarding the comparative effectiveness, and longevity of treatment effectiveness, of different types of psychological intervention that should be recommended to patients. Furthermore, guidelines scarcely provide supporting information to help clinicians and patients decide which psychological approach should be preferentially selected (eg, the particular psychological intervention that is most beneficial for a specific health outcome).19202122 This systematic review provides evidence that the integrated delivery of psychological interventions with physiotherapy care is better than physiotherapy care alone, at least in the short term to mid-term. Available evidence suggests that psychological interventions are safe for this population. Ultimately, the choice of psychological intervention should be selected based on the patient’s primary complaint, concurrent symptoms, and their treatment goals, and should be made in conjunction with the treating clinician. An exploration of the mechanisms by which these interventions improve clinical outcomes for people with chronic LBP is beyond the scope of our review. However, co-delivery of structured exercise and psychological strategies has strong potential to help patients with building resilience and psychological flexibility to better cope (that is, self-manage) with the physical and psychosocial challenges of living with chronic pain.107108
For clinicians
Findings from our review are based on low to high quality evidence. Consistent with psychologically informed practice, an approach described more than a decade ago,109110 our results reinforce the clinical advantages of integrating physiotherapy care with psychological strategies or interventions. Specifically, in conjunction with physiotherapy care, pain education provides the most sustainable effects for improving physical function and behavioural therapy has the most sustainable effects for reducing pain intensity. For fear avoidance, cognitive behavioural therapy with physiotherapy care might result in the most sustainable effects over time; however, pain education delivered with physiotherapy care also results in clinically important benefits of treatment that persist until short term follow-up. Based on a small number of studies, evidence is inconclusive for the effect of mindfulness or counselling based interventions, with or without physiotherapy care, on physical function, pain intensity, and fear avoidance, compared with physiotherapy care. These recommendations are made with consideration of the limited but consistent evidence regarding the safety profile of psychological interventions for people with chronic, non-specific LBP. Given that the largest effects of treatment were found at post-intervention, early screening for the presence of psychological factors in patients with chronic LBP, and integration of both therapies together at the outset of treatment, might help to maximise improvements in patient outcomes.
However, existing patterns in patient access to exercise and psychological therapies for LBP suggest that early integration of both therapies at the outset of treatment might be difficult to implement. Across global healthcare systems, direct access (that is, self-referral) to exercise providers (eg, physiotherapists, exercise physiologists, and chiropractors) or psychological services is not the routine mechanism for patients accessing these types of care.111112 In contrast, patients typically access these services as secondary or tertiary care, via referral from general practitioners.111112 However, a systematic review of usual care for LBP has shown that the rate of referral to physiotherapy after consultation with a family practitioner is as low as 14% to 27%,113 and in the absence of data, we postulate that the rate of referral to psychological services for LBP is even lower. Overcoming the low referral rates to exercise and psychological services, despite evidence for their effectiveness, is a challenge on its own. Furthermore, the current multidisciplinary approach towards health service delivery can impose further barriers towards early integration of both therapies. Results from an Australian survey of patients who had sought primary care treatment for LBP in the preceding year found that 28% of patients consulted between four to eight different practitioners for their LBP.114 Although these findings are alarming, they are not surprising given that exercise providers and psychologists traditionally operate in siloed settings, which can lead to disjointed care. Considering that poor cross disciplinary collaboration can proliferate negative perceptions from the patient about illness, delay recovery, and reduce quality of life in patients with LBP,115 the current multidisciplinary model of care for LBP could be insufficient in meeting patient needs and is likely to be inadequate for supporting effective integration of care.
To optimise co-delivery of exercise and psychological therapies at the onset of treatment, interdisciplinary or intradisciplinary approaches to treatment delivery can be feasible alternatives. In health, interdisciplinary approaches describe the co-ordination of different health disciplines working together to optimise care delivery, whereas intradisciplinary approaches describes single health disciplines blending skills within their own scope of practice, with concepts, methods, or techniques borrowed from other disciplines. The amount of evidence is growing suggesting that, in line with psychologically-informed practice, exercise providers (mainly physiotherapists) have the capacity to successfully incorporate psychological strategies into treatment for patients with musculoskeletal pain conditions.61116117 In clinical psychology, promotion of physical activity and movement are established as inherent components of cognitive behavioural therapy interventions for chronic pain, such as graded activity or graded exposure. A recent systematic review with an NMA of 217 randomised controlled trials has shown that patients with LBP benefit from being encouraged to perform exercises that they enjoy.118 Consequently, psychologists are well situated to potentially incorporate structured exercise programmes, guided by a patient’s preference, into treatment. Overall, we remind exercise providers that incorporating psychological strategies into treatment is crucial for maximising physical function or reducing pain intensity and fear avoidance. We also remind psychologists that exercise is an important component of behavioural therapy or cognitive behavioural therapy, and adjunct to pain education programs. Incorporating exercise into treatment is crucial for optimising clinical improvements in people with LBP. Finally, we remind primary care practitioners that patient referrals should include recommendations for the early co-delivery of exercise and psychological therapies, ideally via an intradisciplinary approach; although, interdisciplinary care involving a coherent and coordinated effort between different disciplines might also be appropriate.
Nonetheless, we recognise that interdisciplinary or intradisciplinary approaches to treatment delivery come with their own challenges. Patients still perceive cross disciplinary care to be fragmented, and organisational support and collaboration between different health professionals is insufficient.119120 Clinician perceived barriers exist regarding the incorporation of psychological strategies into clinical practice, such as insufficient knowledge, concerns with reimbursement, time constraints, and reluctance of patients to engage in these types of treatment.116121 The establishment of integrated cross disciplinary clinical networks or coordinated care pathways, or the provision of sufficient training (eg, multiday workshops co-designed with multidisciplinary input), resources,116121 mentoring, feedback,122 or subsidies for clinicians,123 are potential strategies to overcome these challenges. However, further research involving key stakeholders is needed to better support clinicians, health systems, and ultimately, patients with LBP.
Implications for research
This review has identified a need for higher quality clinical trials investigating the effectiveness of interventions based on behavioural therapy, mindfulness, and counselling for people with chronic, non-specific LBP, as the quality of existing trials is highly variable (eg, small sample sizes). Furthermore, clinical trials with longer follow-up periods, particularly beyond 12 months post-intervention, are necessary to improve evaluation of the comparative long term effectiveness of psychological interventions. In addition, the assessment and reporting of data for health related quality of life and safety across studies of psychological interventions for chronic, non-specific LBP is highly heterogenous and generally absent, which prevented us from performing NMA for both outcomes. For health related quality of life, greater consistency in the measurement instruments used and a better understanding of the recommended administration and scoring procedures for validated instruments could improve our ability to compare findings across future studies. Nevertheless, we recognise that current tools specific for back pain or musculoskeletal conditions are scarce for assessing health related quality of life.30124
We also raise some concerns about the poor quality of safety data reporting. Most studies did not have sufficient information regarding adverse events, for relatedness (that is, whether the adverse event was a direct result of participating in the study intervention), temporality (that is, whether the adverse event occurred during the intervention period or during the follow-up period), severity (that is, mild, moderate, or severe), and independence (that is, most studies reported a total count of adverse events across the entire study population and did not report whether multiple adverse events were experienced by the same participants). A previous review of 82 National Institute for Health Research funded clinical trials investigating psychological interventions has found that adverse events are often assessed according to inappropriate criteria that are not therapy specific.125 Therefore, the development and implementation of standardised reporting guidelines for adverse events that are tailored for psychological interventions might improve accuracy of reporting and synthesising data126 and strengthen the risk-benefit assessment of their clinical value.
Conclusions
This systematic review with NMA investigated the comparative effectiveness and safety of psychological interventions for managing chronic, non-specific LBP. Compared with physiotherapy care alone (mainly structured exercise), psychological interventions are most effective for people with chronic, non-specific LBP when they are delivered in conjunction with physiotherapy care. Although the clinical effectiveness of psychological interventions diminish over time, the most sustainable effects of treatment for physical function and fear avoidance are achieved with pain education programmes. The most sustainable effects of treatment for pain intensity are noted with behavioural therapy. Limited but consistent evidence suggests that psychological interventions are safe for people with chronic, non-specific LBP, and the effects of treatment are maintained at least from post-intervention until the short term to mid-term after treatment. The comparative effectiveness of psychological intervention for improving health related quality of life is unclear owing to heterogeneity of reporting. Ultimately, to optimise improvement in patient outcomes, clinicians should consider strategies to promote early and cohesive co-delivery of structured exercise and psychological strategies or interventions together.
What is already known on this topic
Existing clinical guidelines consistently endorse multimodal treatment approaches, involving exercise and psychosocial therapies, for managing chronic low back pain
Current guidelines provide limited information regarding the specific types of psychological interventions that should be recommended for different clinical outcomes, as well as the comparative longevity of intervention outcomes
The comparative effectiveness of psychological interventions available for managing chronic low back pain is unknown, potentially contributing to patients and clinicians being uncertain regarding the most optimal choice of treatment
What this study adds
This systematic review with network meta-analysis, a statistical method that enables simultaneous comparison of multiple interventions, investigates the effectiveness of psychological interventions for chronic low back pain
Compared with physiotherapy management, the most sustainable effects for physical function and fear avoidance were achieved with pain education programs delivered with physiotherapy care, and for pain intensity was behavioural therapy delivered with physiotherapy care
Findings can help to improve the clarity of guideline recommendations regarding the most effective psychological interventions for this population, to better support patients and clinicians in treatment decision making
Ethics statements
Ethical approval
Not required.
Data availability statement
Requests for data sharing should be sent to the corresponding authors: Emma K Ho (emma.ho{at}sydney.edu.au) or Lingxiao Chen (lche4036{at}uni.sydney.edu.au)
Acknowledgments
We thank the study authors who provided data and additional information for this review. We thank Kanchana Ekanayake (Academic Liaison Librarian) for her support in preparing the search strategy. We also thank several people for providing language support: Fereshteh Pourkazemi (Farsi), Markus Hüebscher (German), Antoine Camus (French).
Footnotes
Contributors: EK-YH and LC (lche4036{at}uni.sydney.edu.au) are joint corresponding authors and contributed equally to this work. EK-YH drafted the manuscript. PHF and MLF share senior authorship. EK-YH, JC, and DXMW contributed to study screening and data extraction. JC and DXMW evaluated the risk of bias within studies. EK-YH evaluated the confidence in the cumulative evidence. EK-YH and LC performed data analysis. EK-YH prepared the graphs and tables. All authors (EK-YH, LC, MS, CEA-J, JC, DXMW, JAH, MLF, and PHF) contributed substantially to revisions of the manuscript, and all authors (EK-YH, LC, MS, CEA-J, JC, DXMW, JAH, MLF, and PHF) approved the final version of the manuscript. EK-YH and LC are the guarantors. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. EK-YH is funded by an Australian Government Research Training Programme Scholarship. PHF and MLF are funded by National Health and Medical Research Council of Australia Research Fellowships. MS is funded by a Sydney University SOAR fellowship. LC is funded by Northern Clinical School Higher Degree Research Support Scholarship.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years, no other relationships or activities that could appear to have influenced the submitted work.
The lead authors (EK-YH and LC) affirm that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as originally planned (and, if relevant, registered) have been explained.
Dissemination to participants and related patient and public communities: We will disseminate our findings to clinician and patient organisations, and through traditional media and social media outlets. Study results will be presented in a variety of national and international conferences and forums.
Provenance and peer review: Not commissioned; externally peer reviewed.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.