Article Text

Abstract
Inappropriate behaviour is an umbrella term including discrimination, harassment and bullying. This includes both actions and language and can affect any member of the cardiovascular workforce/team. Evidence has suggested that such behaviour is regularly experienced within UK cardiology departments, where inappropriate behaviour may represent longstanding cultural and practice issues within the unit. Inappropriate behaviour has negative effects on the workforce community as a whole, including impacts on recruitment and retention of staff and patient care. While only some members of the cardiology team may be directly impacted by inappropriate behaviour in individual departments, a wider group are significantly impacted as bystanders. As such, improving the culture and professional behaviours within UK cardiology departments is of paramount importance. As a negative workplace culture is felt to be a major driver of inappropriate behaviour, all members of the cardiovascular team have a role to play in ensuring a positive workplace culture is developed. Episodes of inappropriate behaviour should be challenged by cardiovascular team members. Informal feedback may be appropriate where ‘one-off’ episodes of inappropriate behaviour occur, but serious events or repeated behaviour should be escalated following formal human resources protocols.
- Quality of Health Care
- Delivery of Health Care
- Education, Medical
- Organizational Objectives
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
This British Junior Cardiologists’ Association (BJCA) and British Cardiovascular Society (BCS) policy statement aims to outline issues related to discriminatory and inappropriate behaviour which is both unprofessional and unacceptable. This behaviour includes bullying, inappropriate language (eg, sexist, racist or homophobic language), discrimination, harassment and inappropriate behaviour towards any member of the cardiovascular workforce. This behaviour can have a direct impact on individual well-being, performance and mental health, and indirectly on wider cardiology service delivery and patient care. All members of the cardiovascular workforce are entitled to work in an environment where appropriate and professional behaviour is the expected standard and episodes of inappropriate behaviour are not tolerated, but challenged when they occur. Key recommendations from this document are detailed in table 1.
Key recommendations and action points for implementation at individual, departmental and national levels
Bullying, harassment and discrimination as inappropriate behaviour
This document uses the term ‘inappropriate behaviour’ as an umbrella term. Discrimination, harassment and bullying are inappropriate behaviours. Such behaviours can affect any member of the cardiovascular workforce. Unconscious biases and previous training role models can underpin the manifestations of these behaviours and interactions with others. Being aware of such biases is a vital first step in combating such behaviour.
Bullying
While individual experiences are inherently subjective,1 The charity Bullying UK defines workplace bullying as:
A form of abusive behaviour where an individual or a group of people, create an intimidating or humiliating work environment for another.2
The NHS specifically outlines a number of other actions and behaviours that constitute workplace bullying3:
Excluding and ignoring people and their contribution
Overloading people with work
Spreading malicious rumours
Unfair treatment
Picking on or regularly undermining someone
Denying someone’s training or promotion opportunities
Bullying may or may not be intentional.1 Individuals may be unaware of the effect their words or actions have on others.4 Such accidental bullying is just as damaging to the individual experiencing it.4 A proportion of individuals who exhibit bullying behaviours may be ‘redeemable’ if they can change these behaviours once a satisfactory way of feeding back to them the effect they have on others is devised. This, alongside robustly tackling more egregious behaviours, represent potential targets for action.
Importantly, we must also consider what bullying is not:
Character building
It is often suggested that this is how cardiologists were trained in the past and that it helps to ‘build character’. This is an anachronistic and flawed concept: intimidating language or actions do not build character and have substantial negative impacts on those affected. Furthermore, role modelling and learnt behaviours lead to perpetuating the cycle of bullying.
Robust feedback
Some individuals may attempt to define the behaviours that are, in fact, bullying as a style of leadership or the way they provide feedback in a stressful situation. Frank feedback is an important aspect of learning.5 However, if this leads to an individual feeling intimidated or humiliated, this is bullying.
This inability to provide feedback in a manner that is considered comfortable and constructive is one of the biggest identifiable challenges. It also represents a clear target for improvement for staff whose feedback style is unsuitable, but who are willing to undergo training.
The victim’s fault
Bullying is not the fault of the bullied. While mistakes happen in medicine and may require frank feedback to aid learning, they are not an excuse for intimidating or belittling behaviour or language.
However, providing essential feedback about suboptimal outcomes and/or performance is one of the most important functions of a trainer and a valuable characteristic of a colleague: the skillset required to carry out this task effectively requires training that is not routinely provided to UK cardiologists and members of the wider cardiology team. This may represent another target for departmental improvement action.
Other inappropriate behaviour, language and actions
As professionals, all members of the cardiovascular workforce should communicate and act inclusively with each other using respectful language and actions. Examples of inappropriate language include (but are not limited to) sexist, homophobic, or racist language and unconstructive negative comments on performance. Inappropriate actions include providing or depriving individuals of opportunities based on personal characteristics rather than performance. Episodes of uncontrolled anger, especially recurrent, are also clearly inappropriate and carry a high potential to intimidate. These behaviours impact on all members of the cardiology team and their ability to provide an effective cardiac service.
Discrimination
While bullying is not against the law, discrimination based on a protected characteristic (including age, disability, pregnancy/maternity, race, religion, sex/gender or sexual orientation) is illegal (UK Equality Act 2010).6 Discrimination may be direct or indirect and may result in disciplinary action from the employer.
Harassment
Harassment is when bullying or other unwanted behaviour is about a protected characteristic (age, disability, race, religion, sex/gender or sexual orientation) and either violates the individual’s dignity or creates an intimidating/hostile/offensive environment.6 The intent of the individual undertaking the behaviour is not relevant. Incidents of bullying, whether intended or not, may in fact end up being considered harassment.
While overt discrimination, harassment and bullying can often be easily identified where these manifest, more insidious low level covert language and actions should also be recognised as impacting on the cardiology team and patient care.
Scope of the problem
Bullying
Inappropriate behaviour in UK cardiology departments is common. Bullying was reported by >10% of trainees in the 4 weeks prior to being asked between 2017 and 2020.7 This is supported by data from the General Medical Council trainee survey which suggests that bullying in cardiology is almost double the average across all medical specialties (12.3% vs 6.9%).8 While bullying is a national problem, there is substantial regional variation in the rates of bullying reported by trainees.7 Women and those attending non-UK medical schools are at a greater risk of bullying, a pattern that is also present outside of cardiology.9
Inappropriate behaviour is also frequently experienced by consultants, with 20% reporting being bullied or harassed and 35% reporting feeling undermined at work.10 Women and ethnic minority consultants were more likely to report feeling undermined. The rates of bullying among other members of the cardiovascular workforce are less well established. However, there is evidence that bullying is indeed commonly experienced by nurses and other allied health professionals.11 12
The extent of bullying within UK cardiology has been illustrated over repeated annual surveys. However, while the scope of bullying in UK cardiology is clear, current data do not provide evidence on the extent of the problem in the UK compared with other countries.
Other inappropriate language/behaviour
Further evidence from trainees suggests that both sexist and racist language are common in cardiology departments.7 Women are more likely to report encountering sexist language while those attending non-UK medical schools are more likely to report exposure to racist language. Sexual harassment has been shown to be a significant issue within surgical specialities in the UK,13 and a similar picture has been shown in cardiology.14 15 Other inappropriate behaviours are also relatively common with 9% of trainees reporting being exposed to spontaneous rage/anger.7 The experiences of other members of the cardiology team are not well documented at present. However, it is reasonable to expect that nurses, physiologists and the wider cardiac team have witnessed and been affected by similar behaviours reported by trainees.
Role of professional societies in combatting inappropriate behaviour
Inappropriate behaviour can affect any individual within the cardiovascular workforce. Professional societies have a key role in setting the standard of appropriate care within the specialty. As with clinical standards, professional societies have a role in developing a standard for appropriate behaviour and a responsibility to ensure that inappropriate behaviour is shown to be unacceptable. The development of this document is in line with those produced by other professional societies.16
Why action on inappropriate behaviour is needed
Effects on the cardiology community
Inappropriate behaviour, language and actions have negative impacts across the cardiology team. Workplace bullying has been shown to be associated with a number of negative outcomes, including lower performance, lost productivity and absences.1 Bullying accounts for 50% of stress-related workplace illnesses. Additionally, bullying is associated with an increased risk of serious medical error.17 Those who are bullied are more likely to plan to reduce their working hours or cease patient care.18 Importantly, bullying has wider consequences beyond just the individual being bullied and can negatively impact bystanders19 and patients.20 While the majority of research in this area has focused on cardiologists or cardiologists in training, it would be expected that such effects would be mirrored across the wider cardiovascular workforce. Many members of the cardiovascular community work in services on a long-term basis and can be impacted by either being directly subject to inappropriate behaviour or through indirect observation. These findings highlight that inappropriate behaviour has a significant negative impact on individual practitioners and the wider cardiology community.
Effects on recruitment and retention
Inappropriate behaviour can have an impact on the recruitment and retention of staff across the cardiovascular workforce. Evidence of inappropriate behaviour reduces the attractiveness of the specialty to those considering cardiology as a career.21 22 At a national level, this is likely to continue to impede recruitment of women into cardiology that, as a specialty, already substantially under-recruits women, and where women are less likely to complete cardiology training than their male counterparts.23 24 At a local level, departments with a reputation for poor professional interactions are less likely to attract the best candidates for roles in their departments including skilled nurses and allied health professionals that are required for departments to operate. Evidence suggests that departments that improve workplace culture can improve staff retention rates.4
Effects on care, patients and patient experience
I am in no doubt that bullying is a problem that urgently needs to be addressed. It has implications for patient safety, for staff morale, for performance, and for staff retention.
Sir Robert Francis QC (Chair of Healthwatch England)
Exposure of patients to inappropriate behaviour can lower patients’ confidence in the quality of their treatment and undermine their trust in their treating team.25 Given that most interventional and diagnostic procedures in cardiology are performed on conscious patients, the risk of patients being exposed to such behaviour is likely to be greater than in surgical specialties. Loss of patient trust is associated with worse outcomes.26 Specifically, departmental cultures that promote/endorse/allow bullying have been directly associated with worse patient outcomes.4
The patient just like the trainee can feel unheard, humiliated, [and] afraid to speak out or voice their concerns. The result [is] a confused, disheartened frightened patient, they don’t know who to trust and there is an erosion of the relationship with the trainee. The patient doesn’t feel listened to and important clinical information can be missed potentially leading to an incorrect diagnosis and delayed treatment.
Sarah Brown, Lay Representative, Cardiology Specialist Advisory Committee
Bullying has financial consequences due to the costs related to staff loss and absences. Improving standards of professional behaviour, communication skills and the resulting patient experience has also been shown to increase departmental and individual practitioner revenue.27 28
One thing that worries me more than anything else in the NHS is bullying.
Sir Ian Kennedy, Chair Bristol Royal Infirmary Report
Inappropriate behaviour broadly—and bullying specifically—have been highlighted as issues in a number of previous reports. The failure to provide appropriate care alongside patient mistreatment and neglect in the Mid Staffordshire NHS Foundation Trust scandal led to the initiation of a public enquiry.29 The Francis Report, resulting from this enquiry, specifically highlighted that reports of bullying towards trainees were not investigated and that there existed a culture of bullying more generally within the Trust.29 Bullying and discrimination are further associated with patient safety through their influence on burnout.30 Bullying cultures have repeatedly been identified in a number of other independent inquiries/reports examining NHS trusts, departments and practitioners.31–33 Disruptive and inappropriate behaviours have been repeatedly linked with lower quality of care.34
Effects on healthcare organisations
In addition to the effects outlined above which have both direct and indirect effects on healthcare organisations, bullying and harassment increases costs for healthcare organisations. In particular there are direct costs related to absenteeism and requirement to obtain replacement staff.35 There are indirect costs which relate to decreased performance and reduced quality of patient care in departments where bullying and harassment occurs.35
What tackling inappropriate behaviour should not prevent
Constructive feedback is important for learning. Consultants and other team members should not avoid providing ‘negative’ feedback when required. Indeed, negative feedback delivered in good faith and in a constructive manner is a vital learning tool. Such feedback should be delivered professionally, with the aim of improving performance, and linked directly to a specific training outcome or objective. One of the key improvement action targets must be to help individuals to acknowledge the importance of them taking responsibility for delivery of feedback in a manner that is considered acceptable to the person receiving it, regardless of the culture they are used to.
Drivers of inappropriate behaviour
Inappropriate behaviour may reflect cultural issues within the department/hospital/region rather than the individual. Inappropriate behaviours may also be influenced by unconscious biases or may be a manifestation of stress, workload pressure and/or deteriorating mental health. As such, individuals may be unaware that episodes of behaviour are inappropriate. While individuals must be accountable for their behaviour, department culture is inherently responsible for allowing it to continue. Establishing a positive culture, rather than punishing individuals, must therefore be the central focus of tackling inappropriate behaviour.
Senior members of cardiology departments, including but not limited to cardiology consultants, are role models for the rest of the cardiology team. Other colleagues observe how senior members behave and act. As such, inappropriate behaviour from senior team members can lead to learnt behaviour from other members of the cardiology team.
Evidence suggests that bullying is more prevalent in stressful work environments.36 This in turn can result in greater levels of workplace stress for individuals,37 resulting in a cyclical deterioration in the workplace environment. System-wide pressure to meet targets may exacerbate stress for both individuals and departments and result in an increase in inappropriate behaviour.38 An over-focus on targets has been highlighted as an underlying factor in the Mid Staffordshire NHS Foundation Trust scandal.39
Intervention to manage behaviour: informal and formal
In some cases, inappropriate behaviour is of such an egregious level or represents a defined pattern, despite informal interventions, that escalation and formal reporting to a person of authority within the department and/or human resources is required. In such cases, appropriate investigations and outcomes should be both documented and follow formal management processes, with support for all parties. However, in other cases where individuals are not persistent users of inappropriate language or behaviour, intervention should initially focus on education and awareness in an informal setting. Starting initially with authority-based intervention may not be necessary in all cases and may have negative effects on both the individual and the departmental culture. It is, therefore, unlikely to deal with the cultural issues that allow such behaviour to exist or flourish. Such a systems/culture approach has been put forward in the Freedom to Speak Up report.4 However, in situations where an individual continues to exhibit inappropriate behaviour or use inappropriate language despite an initial informal approach, more formal mechanisms must be employed. Such formal mechanisms should involve the human resources team; the specifics of formal intervention will depend on local policies within individual workplaces and the specifics of the behaviour reported.
Inappropriate and unprofessional behaviour between specialties
Inter-specialty interactions are also an area where inappropriate and unprofessional behaviour is common. For example, unprofessional behaviours (such as being rude during discussions with another specialty) displayed by some cardiology registrars have been cited as contributing towards a negative view of the specialty.22 These must be recognised and should be tackled in the same way as any other form of inappropriate behaviour in the department. How we treat other specialties reflects on the cardiology team as a whole and can quickly become the standard we tolerate when communicating within the specialty or department. This reputation is highly likely to discourage individuals from entering cardiology as a specialty or the wider cardiovascular workforce, and impact on inter-speciality working for the best interests of our patients.
Academic cardiovascular medicine
Inappropriate behaviour within research environments is common and must also be acknowledged. Senior academics are role models for early career researchers including trainees, allied health professionals and others within academia, as well as those undertaking higher research degrees. Individuals working in academic and research environments often feel they have limited power when experiencing inappropriate behaviour from seniors. While the same requirements to be able to provide criticism exist as with clinical medicine, this must be done professionally. Funders and universities must ensure that professional behaviour is a requirement for funding and advancement within cardiovascular research and that prior findings of inappropriate behaviour are considered as part of evaluation processes. Universities should also ensure that appropriate mentors and advisors outside of the direct supervisory chain are available to everyone taking part in cardiovascular research to ensure that there are alternative avenues available to those who are subject to inappropriate behaviour from supervisors.
Responsibilities to speak up
Individuals who are bullied are often unaware that what they are experiencing would be considered bullying.7 Furthermore, individuals who are bullied often feel intimidated and fear repercussions for reporting bullying behaviour.1 As bullying is a cultural issue, all of us within that culture are responsible for allowing or perpetuating that behaviour. As a result, everyone within a cardiology department has a responsibility to highlight and manage inappropriate language or behaviour. Witnessing inappropriate behaviour/language and ignoring it perpetuates the behaviour and is how poor workplace culture develops.
The standard you walk past is the standard you accept.
General David Morrison (Chairman of the Diversity Council Australia)
However, while we all have responsibilities to tackle poor workplace culture, not everyone will feel that they have sufficient power to directly confront the individual. In those situations, such inappropriate behaviour should be raised with someone who is in a position to act, and departmental policies should clearly outline processes for reporting these concerns.
Responsibility to respond
Leaders within cardiology departments have a responsibility to respond seriously and promptly to reports of inappropriate behaviour.20 While informal approaches to resolution in such settings may be appropriate, individuals reporting inappropriate behaviour have a right to be supported by their hospital trust, department and individuals within the department. Departments should have a defined and transparent protocol for dealing with reports of inappropriate behaviour, including how they are investigated and a consistent policy for determining outcomes.
Knowing what’s right doesn't mean much unless you do what’s right.
Theodore Roosevelt (US President, 1901–1909)
Whistle-blower protection
Individuals who report inappropriate behaviour should not be targeted or face negative consequences as a result of raising issues. This has been repeatedly highlighted as an issue within medicine and the wider healthcare environment, and substantially limits the willingness of individuals to raise issues about inappropriate behaviour.4 Department policies for dealing with inappropriate behaviour must therefore include systems to safeguard individuals raising concerns.
Evidence to suggest individuals may cynically attempt to manipulate such systems is limited.4 While deliberately raising a false allegation is never acceptable, in the absence of additional evidence, those raising a concern must be treated from the outset as though the allegation is genuine and the department’s standard policy for dealing with such reports should be followed.
Approaches to tackling inappropriate behaviour
Promotion of positive workplace culture
All individuals, departments and national bodies are responsible for promoting a positive workplace culture (figure 1). Departments and national bodies should establish clear standards and expectations of behavioural norms from all members of the cardiovascular team. When considering promotions and leadership roles, departments should consider any incidences of inappropriate behaviour in the selection process. National bodies should take into account past patterns of inappropriate behaviour when considering individuals for roles within their organisation, at meetings, or the presentation of awards.

Promoting workplace culture and awareness through a British Cardiovascular Society anti-bullying campaign.
Zero-tolerance policy
Bullying within cardiology departments is unacceptable and has no place in modern medical practice. A zero-tolerance approach to bullying and harassment is endorsed by the General Medical Council and British Medical Association with recourse for robust action where required.40 41 However, it is also accepted that the extent and intent of bullying can differ. As such, while all bullying is unacceptable, the actions for managing those that bully must take into account the context of the actions.
Having a zero-tolerance policy for accepting such behaviour therefore does not equate to an automatic need to punish individuals. Where appropriate, informal or formal education may be a reasonable initial course of action, particularly, for example, those who undertake isolated episodes of inappropriate behaviour unintentionally and seek to engage positively when challenged.
Unconscious bias and workplace culture training
Given the potential for unconscious biases to be factors in inappropriate behaviour, all members of the cardiology team should have regular unconscious bias training to improve awareness of these drivers of behaviour. While the evidence is mixed, unconscious bias training has generally been shown to be effective for reducing—but not eliminating—such biases.42 All members of the cardiovascular workforce should have regular training on workplace culture which should include recognising and dealing with inappropriate behaviour at work. There is no clear evidence on the frequency of training required. While annual training would seem a sensible minimum, the exact frequency should be determined locally. This training should be delivered to the whole team together wherever possible, rather than individually, as this has been shown to improve effectiveness.43
Training in feedback
The giving and receiving of feedback has been reported as a perceived potential flashpoint for inappropriate behaviour within cardiology. It is imperative that a system for training cardiology team members is developed to ensure that they are educated in the delivering (and receiving) of structured and appropriate feedback.5 Cardiology departments should ensure that such training is easily and freely available to all current team members and new members should be expected to undertake such training when joining the department. Courses are currently available from the Royal College of Physicians,44 the British Medical Association,45 and others. This will allow those delivering feedback to feel confident that they are doing so in an appropriate and constructive manner.
Human factors training
Given the potential association between stressful work experiences and inappropriate professional behaviour, cardiology-specific human factors training should be made available in all cardiology departments. Human factors training aims to improve communication skills and behaviour within teams.46 Such training has been shown to improve patient outcomes,47 and has an extensive history within aviation. Further, for the well-motivated and redeemable individual, bespoke training in acquiring new skillsets for interacting with colleagues could be extremely effective. Such training should be made available to all members of the cardiovascular workforce as part of routine organised mandatory training and development. New team members should be expected to undertake such training when joining the department as part of their formal induction. Such courses are available from a range of bodies including NHS trusts48 and the airline industry.49
Professional behaviour lead
All cardiology departments should designate a professional behaviour lead who can act as a central person to whom members of the cardiology team can report inappropriate attitudes, language or behaviour. This could be an individual from outside the department who can provide an external perspective and an objective arbiter when allegations of inappropriate behaviour are made.
The professional behaviour lead should be trained to investigate and manage allegations of inappropriate behaviour following an agreed departmental policy. This would include ensuring that those found to have undertaken inappropriate behaviour receive appropriate training. They would also keep track of allegations to allow patterns of behaviour to be recognised. They should report back regularly through local and regional feedback loops. Additionally, as part of a duty of candour, the professional behaviour lead would be expected to keep those who have alleged inappropriate behaviour towards others up to date on the progress and outcomes of investigations. At any point, the professional behaviour lead may involve the human resources team or the local Trust’s Freedom to Speak Up Guardian if required. Freedom to Speak Up Guardians are specific roles which aim to facilitate trust employees to report issues including inappropriate behaviour and will have familiarity with the trust policies and protocols for doing so.
UK cardiovascular national bodies should similarly ensure that there is someone within their leadership structure who is tasked with promoting professional standards and a positive culture.
Model for change
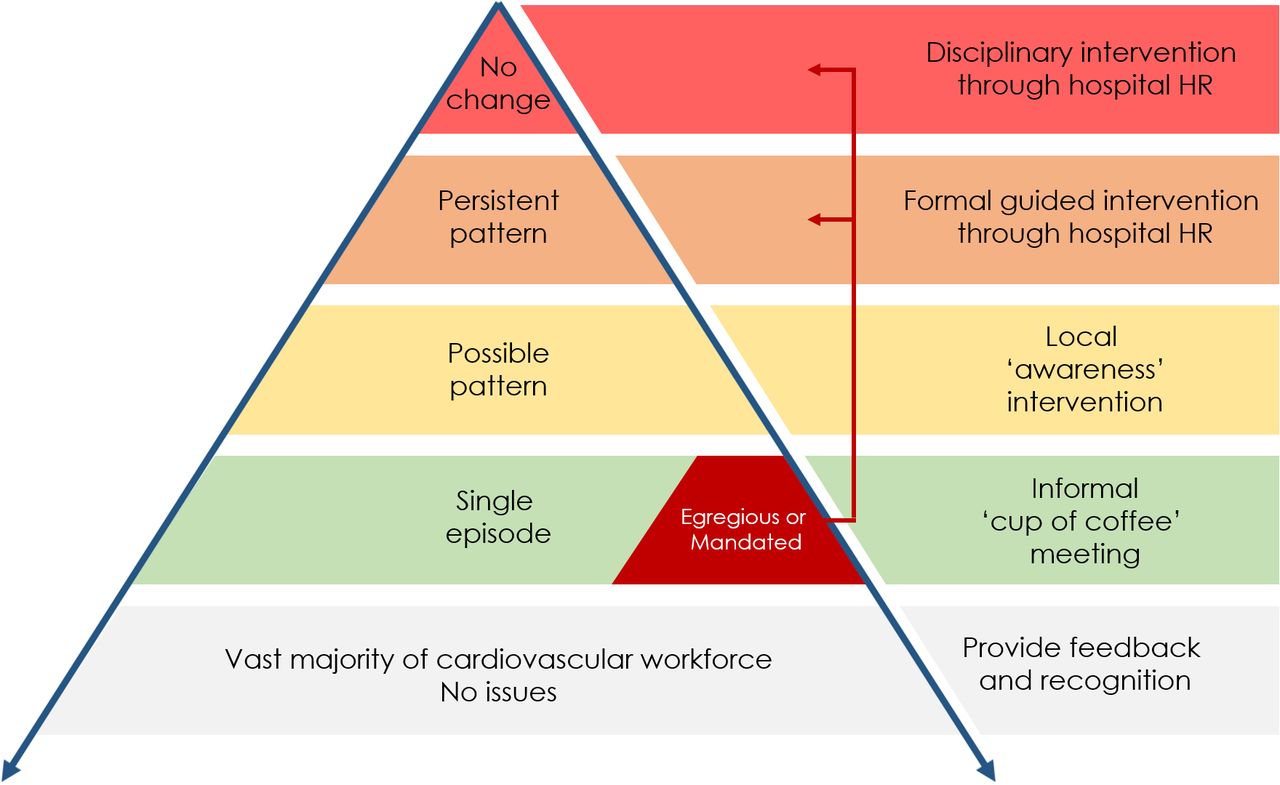
As individuals who undertake inappropriate language or behaviour may do so unknowingly, interventions should initially aim to inform individuals of where their behaviour has fallen below the expected standard. This can be achieved using the ‘cup of coffee’ model (figure 2),50 51 with more formal approaches undertaken if there are repeated incidents leading to a pattern of behaviour.41
{kind=link}
{kind=link}
Promoting professionalism pyramid. Adapted from Hickson et al. 51
Isolated episodes of inappropriate behaviour should be used as a learning experience for the individual with feedback delivered in an informal setting (for example, over a cup of coffee). Feedback should be clear about the problem their behaviour has caused, but offer the chance to improve using appropriate training, thereby offering a constructive improvement action. In some cases, for example, the approach should take the same pathway of feeding back about suboptimal performance as they would be expected to use for trainees and other members of the cardiovascular workforce.
Such informal feedback may be undertaken by the individual who feels they have been affected by inappropriate behaviour directly. However, some will not feel this is possible, feasible or appropriate. As such, another individual or the departmental professional behaviour lead may undertake the intervention, either acting jointly with the affected person or separately.
It is likely that members of the cardiovascular workforce who undertake isolated incidents of inappropriate behaviour do so without clear insight. Indeed, many may be upset to discover they have behaved this way. Of individuals who receive such feedback, a substantial proportion may be motivated to improve their behaviour. Furnishing them with constructive feedback and advice/training may facilitate real change in the ‘redeemable’ group. Such feedback should be supplemented by routine use of multi-source feedback where evidence of both good and inappropriate behaviour can also be raised.
Inherently, some behaviour or language may fall far below the expected standard that will require more formal intervention immediately. Additionally, those who engage in repeated episodes of inappropriate behaviour despite appropriate informal intervention must be recognised and more formal interventions undertaken. If internal interventions within the department fail, such individuals should be escalated outside of the department through established NHS Trust-based HR pathways.
National reporting strategy
Individuals must be encouraged to report inappropriate behaviour locally and to escalate using the model outlined above. However, a national cardiology reporting strategy is required to ensure that members of the cardiovascular workforce who are subjected to, or witness, bullying behaviour are able to report it without fear of repercussions. Such a national reporting system does not aim to ‘name and shame’ individual practitioners or institutions but instead to provide an overview of regions/hospitals/departments with ongoing cultural issues related to inappropriate behaviour. Within NHS Trusts, Freedom to Speak Up Guardians should be incorporated into this strategy and work locally to support individuals and departments.52
Saying sorry
Cardiology, at a specialty and departmental level, must normalise individuals apologising for inappropriate behaviour. Indeed, it is likely that many isolated episodes of inappropriate behaviour, if recognised, could be rectified by the individual if they apologised for and reflected on their actions. Someone providing an appropriate apology should acknowledge what has happened and admit that they made a mistake as well as concentrating on what they’ve learnt and would do differently moving forward. The words ‘I’m sorry’ are important and non-apology apologies should be avoided.
Conclusions
Cardiology as a specialty has a high prevalence of inappropriate behaviour, which suggests an endemic cultural issue within many UK cardiology departments. Such behaviour has negative consequences for patients and staff, either directly or as bystanders. Inappropriate behaviours have repeatedly been highlighted in reports/inquiries into poor standards of NHS care.
Individuals must be supported in reporting inappropriate behaviour and departments must develop a responsive attitude to dealing with such reports. While some behaviour may require formal action immediately, others may be tackled initially by informal approaches that raise awareness and provide education to change behaviour with more formal action reserved for those who demonstrate a pattern of behaviour.
While individuals may be responsible for their own behaviour, it is the culture that cardiology as a specialty allows to develop that facilitates and endorses such actions. As such, cultural change is required and must be undertaken to tackle this problem.
We have highlighted a number of improvement actions that may facilitate change by engaging colleagues responsible for such behaviours in a manner that could help those motivated to improve to acquire a new interactive skillset. Addressing this issue in as constructive a manner as possible, while highlighting and stopping serial offenders, will preserve the essential work that the majority of individuals within the cardiovascular workforce achieve.
Top take home messages
Bullying and other forms of inappropriate behaviour/language are common within UK cardiology departments and can affect any member of the cardiovascular team.
Such inappropriate behaviour has a material impact on the cardiovascular workforce community and patient care.
As a community, members of the cardiology team have a responsibility to speak up about inappropriate behaviour and a responsibility to respond.
Informal approaches including education and support may be suitable for individuals as a first step in addressing inappropriate behaviour where this is believed to be an isolated episode.
A number of strategies are required at the departmental, regional and national level to improve the culture within UK cardiology.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
Twitter @cfcamm, @theharveys, @ncurzen
Collaborators Endorsing Organisations: British Cardiovascular Society (BCS), British Junior Cardiologists Association (BJCA), Association for Inherited Cardiac Conditions (AICC), British Association for Cardiovascular Prevention and Rehabilitation (BACPR), British Association for Nursing in Cardiovascular Care (BANCC), British Atherosclerosis Society (BAS), British Congenital Cardiac Association (BCCA), British Cardiovascular Intervention Society (BCIS), British Cardio-Oncology Society (BC-OS), British Heart Rhythm Society (BHRS), British Heart Valve Society (BHVS), British Nuclear Cardiology Society (BNCS), British Society of Cardiovascular Imaging (BSCI), British Society of Cardiovascular Magnetic Resonance (BSCMR), British Society for Cardiovascular Research (BSCR), British Society of Echocardiography (BSE), British Society for Heart Failure (BSH), Cardiovascular Care Partnership UK (CCPUK), Primary Care Cardiovascular Society (PCCS), Society for Cardiological Science and Technology (SCST), UK Maternal Cardiology Society (UKMCS).
Contributors All authors contributed to the preparation, critical review and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.