
Abstract
Over the past decade, it has become clear that the health sector is not only at risk from climate change but also a major polluter of greenhouse gases. In November 2021, the World Health Organization and partners launched the COP26 Health Programme for sustainable, climate-resilient and low-carbon health systems, and have since established the Alliance for Transformative Action on Climate and Health to support its implementation. Given the wide variation in health financing, carbon emissions and unmet health needs across the world, fair sharing of the remaining carbon budget and health gains will be critical. In this Perspective, we explore the challenges and opportunities of healthcare decarbonization, outlining the principles of fair pathways to net-zero healthcare that are attentive to health and socioeconomic inequalities within and between countries.
Similar content being viewed by others

Main
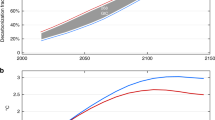
The growing awareness that the health sector is not only at risk from the impacts of climate change but also a major polluter—responsible for 5.2% of global emissions1—has spurred an international, grassroots movement for low-carbon healthcare. Time is rapidly running out to limit global temperature rise in line with the Paris Agreement, the intergovernmental treaty to limit temperature rise to below 1.5–2 °C. Even the upper 2 °C limit requires a 5% net reduction in emissions this year—on par with the impact of the coronavirus disease 2019 (COVID-19) pandemic on emissions in 2020—ratcheting up to 17% per year by 2050 (Fig. 1). Meanwhile, staying below the lower 1.5 °C target, with even a one in two chance, requires a transformational 50% reduction in emissions by 2030—reaching net zero by 2050 (ref. 2). It is now widely understood that to stand any chance of meeting these targets, every organization, across every sector, everywhere, needs to do its part; healthcare is no exception.

This highlights the importance of early action to mitigate carbon emissions. The thick black line shows actual historical emissions. Dashed colored lines show past and future trajectories, respectively, to limit warming to 2 °C, starting in different years. Each curve reflects a >66% chance of staying below 2 °C using carbon budgets from the IPCC SR15 report60. This figure by Robbie Andrew is licensed under CC BY 4.0 (ref. 61).
At a global level, health sector decarbonization is currently coordinated under the World Health Organization (WHO) COP26 Health Programme, launched at the COP26 climate summit in November 2021 (ref. 3), with its implementation supported by the recently established Alliance for Transformative Action on Climate and Health (ATACH)4. To date, 58 countries from across all world regions and income groups have committed to developing a sustainable low-carbon health system, of which 22 countries have set a specific date to reach net zero5. While net-zero healthcare is a shared target, the challenges facing policymakers differ markedly across the world. In high-income countries, healthcare carbon emissions have already decoupled from spending, driven by wider societal decarbonization6; in England, emissions fell by a quarter between 1990 and 2019, while health budgets tripled, service utilization doubled, and the population grew by a fifth7. By contrast, in low-income and middle-income countries, emissions have risen with increases in healthcare spending, service coverage and population size6. The net-zero healthcare agenda raises new challenges for healthcare systems, which have traditionally focused on health outcomes, cost containment and service coverage, with little attention to the climate.
Healthcare’s carbon footprint primarily reflects the availability, access and quality of healthcare in a country, especially secondary care, as well as the makeup of the domestic energy system and healthcare expenditure6,8. The highest proportion of emissions come from global supply chains, highlighting a problem of controlling the carbon footprint as well as the potential value of international collaboration9. Emissions are not, however, equally shared: healthcare carbon footprints vary from below 0.1 tonnes per capita across most low-income countries to almost 2 tonnes per capita in the United States (which represents 25% of healthcare’s global carbon footprint)10,11. On a global, equal fair share basis, 2 tonnes per capita spent on healthcare alone in the United States almost breaches the total per-capita emissions required by 2030 to stay below 1.5 °C (ref. 12).
The principle of a fair distribution of emissions, between people and across time, has consensus in principle, but is little implemented in practice. At present, countries that score high on the social measures of human well-being underpinning the Sustainable Development Goals also breach more critical earth support systems, including a stable climate; this is unsustainable at a global scale13. A critical challenge for health policymakers is, therefore, identifying how to cut emissions while expanding access to quality healthcare. Specifically, given the major differences in healthcare emissions and service provision across the globe, what do fair pathways to low-carbon healthcare look like?
International and intranational justice
International justice
Since the International Panel on Climate Change (IPCC) was established in 1988, the fair division of responsibility for cutting emissions has lain at the heart of global negotiations. Yet, annual emissions have since risen by half, driven by an unequal world. The lowest emitting 50% of the global population is responsible for 16% of this growth and the highest emitting 1% is responsible for 21% of this growth14. Climate change is also independently increasing global economic inequality, substantially increasing the energy requirements of achieving decent living standards and health for all15, in even the most optimistic climate mitigation scenarios16. Yet, given existing inequalities, effective climate mitigation policies can also have unfair outcomes, burdening those who bear least responsibility for the problem. For example, making polluters pay to emit carbon (in other words, ‘carbon pricing’) could, in the absence of progressive financial redistribution, push an additional 50 million people into extreme poverty by 2030 (ref. 17). In spite of widespread political and public consensus on the need for effective and fair climate action18 and the rhetoric of ‘building back better’ after the COVID-19 pandemic, emissions recently rebounded to an all-time high. This needs to change.
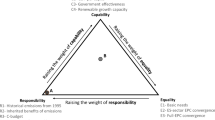
For countries, businesses and sectors (including healthcare), carbon budgets—the cumulative carbon emissions corresponding to a given temperature rise—have been a useful concept to guide and inspire climate action. Precisely how to divide the remaining carbon budget fairly among countries remains more contentious. Different approaches to reducing emissions considered by the IPCC include strategies accounting for historical emissions, the ‘equal per-capita’ view, the capability to reduce emissions and combinations of all three. Each of these is contingent on value judgments19,20,21; as the IPCC states, how costs and benefits are balanced is ultimately ‘a matter of ethics’22.
The common practice of setting targets based on current or prior emissions levels (known as ‘grandfathering’) implicitly excludes the need to consider the factors shaping current emissions, the role of emissions in meeting future development needs and the historical responsibility of polluters23. It is an approach generally considered to be pragmatic but unfair24. The equal per-capita view (or ‘emissions egalitarianism’) is a rights-based approach starting from the premise that, within the context of a finite carbon budget, no one has a greater claim to emit than anyone else. It is often conceived as a tradable permit to ensure that the benefits are progressively distributed from rich to poor. While this view addresses many of the concerns leveled at grandfathering, it has been politically unfeasible to implement25. The capability approach, our focus here, aims to reconcile unequal social and economic conditions with the global common interest. This approach is enshrined in the United Nations Framework Convention on Climate Change, and the Paris Agreement, which emerged from it, under the principle of ‘common but differentiated responsibilities and respective capabilities’ (CBDR-RC)26. It has the potential to address many of these fairness concerns, but requires careful scrutiny; in practice, the lack of a clear operational definition of CBDR-RC has seen countries implement the principle to best suit their self-interests, undermining internationally agreed targets24.
Fair burden sharing presents a new conceptual challenge for the healthcare sector. As illustrated in Fig. 2, healthcare carbon footprints are disproportionately high in rich countries, while the health impacts of climate change are concentrated among the poorest countries. At the same time, lower-middle-income countries also make a substantial contribution to the global healthcare footprint, albeit relatively little as a proportion of global population. When considered within the wider context of improved living standards, life satisfaction and opportunities for all13,15, it is clear that achieving net-zero healthcare globally will be contingent on the trajectory of middle-income as well as high-income countries and that fairness is a vital concern.

This shows that countries with lower healthcare carbon footprints (y axis) are more highly vulnerable to the impacts of climate change (x axis). Width of the circles reflects the proportion of global healthcare emissions (orange) and the proportion of the global population (green) for each income group. Healthcare carbon footprint data are sourced from Lenzen et al.8; climate vulnerability data are from the Notre Dame Global Adaptation Initiative62; population and income data are from the World Bank data portal (https://data.worldbank.org/).
One conceptual hurdle for policymakers is that healthcare is organized and delivered at the national or subnational level with the scope of concern limited, near exclusively, to individuals within the health system—meaning that although cutting emissions is a global good, the direct benefits of cutting emissions to a health system itself may be relatively small. This reflects a tension between ethical responsibilities, which are often global in scope, and political responsibilities, which are generally limited to fellow citizens27. The nature of climate change as a moral problem challenges foundational ethical principles28, which the health sector must also address head on29.
Intranational justice
While cross-country comparisons present a useful analytical frame for fair pathways to net zero, within-country comparisons also have an important role in a world markedly different from when the IPCC was founded. Whereas in 1990 the average citizen in high-income settings had far higher emissions than people in low-income and middle-income countries, today two-thirds of the global inequality in emissions is due to inequalities in emissions within, rather than between, countries14. As shown in Fig. 3, the lowest 50% of emitters in the United States are responsible for similar emissions as the middle 40% in East Asia and Europe and the top 10% in South and Southeast Asia. This highlights a limitation in basing trajectories to net-zero healthcare solely on a country’s per-capita gross domestic product (GDP)30.

This shows large inequalities in per-capita carbon emissions (top 10%, middle 40%, bottom 50%). It also shows that high emissions within regions are driven by the top 10% of emitters, while the lowest 50% of emitters in all regions—including North America and Europe—are currently around or below the per-capita emissions consistent with a 2 °C pathway. Width of the circles corresponds to the proportion of global emissions within each region’s population-income group. 2 °C consistent pathways are from the UN Emissions Gap report12. This figure adapted from the World Inequality Report 2022 is licensed under CC BY 4.0 (ref. 14).
It seems likely that healthcare emissions will display a similar pattern to the inequality of carbon footprints within regions illustrated in Fig. 3, with a relatively small proportion of the population accounting for a large proportion of emissions. This is especially relevant in places with unequal access to quality healthcare, which includes wealthy nations such as the United States, as well as middle-income countries where two-thirds of the world’s poor live31. In countries with publicly funded, universal healthcare systems, this inequality is more indirectly reflected in the relative contribution of healthcare to an individual’s carbon footprint. In England, for example, healthcare emissions are estimated to represent one-fifth of an individual’s carbon footprint in the poorest decile, compared to one-fiftieth in the richest decile32.
Low-carbon healthcare is not simply about international justice, it is also a matter of intranational justice. An increasingly pressing challenge facing healthcare policymakers, administrators, clinicians and ultimately patients, is how to prioritize achieving net-zero ambitions in the face of so many other competing concerns and fairly share the burden and benefits along the way.
Priority setting and net-zero healthcare
Priority setting in health is a process aiming to achieve established goals in an efficient and fair way, and it provides a useful framework to examine pathways to net-zero healthcare. The key ideas underpinning priority setting are: (1) scarcity—that is, demand for a good (for example, health services) exceeds supply, and (2) opportunity cost—that is, choosing one alternative means the loss of other alternatives. Ethical decision-making aims to help balance the competing concerns (‘trade-offs’) facing policymakers, including meeting healthcare needs, reducing out-of-pocket expenditure, and fairly distributing the costs and benefits in a way that expresses the values of individuals and society as a whole33. Priority setting has been widely used in healthcare across high-income, middle-income and low-income settings33. Given the growing commitment to low-carbon healthcare systems, including within ATACH and parallel commitments from G7 Health Ministers34,35, an increasingly pressing question for health policymakers is how to value reductions in carbon emissions in decision-making? There are three foundational issues informing the response.
Firstly, emissions impose harms on others, which needs to be justified, and ideally compensated. Based on Bressler’s analysis of the mortality cost of carbon35, reducing healthcare’s carbon footprint by half this year could avoid 226,000 deaths over the period 2020–2100 from heat-related mortality alone. These deaths probably represent a small proportion of all-cause excess climate-related mortality, concentrated in low-income and low-middle-income countries, which also have the lowest emissions. As discussed by the IPCC, the harms caused by climate change may be partially compensated through adequate climate adaptation funding to those affected; however, these harms cannot be compensated through potentially even greater benefits accruing to polluters (such as high-emitting healthcare systems)22.
Secondly, all emissions are not equal—to whom the benefit occurs also matters. For example, while poverty alleviation will increase the mitigation effort required to stay below 1.5–2 °C (ref. 36), this directly benefits the global poor. Mitigating climate change while eradicating poverty is rightly enshrined in the Paris Agreement37. The philosopher Henry Shue draws a distinction between ‘subsistence emissions’, those necessary to secure basic subsistence, which should not be sacrificed, and ‘luxury emissions’ beyond this level, which should be sacrificed38. Deriving a benefit, even a health benefit, does not mean this represents a source of subsistence emissions. Healthcare interventions with a relatively small marginal health benefit can still have a very large carbon footprint, especially in high-income contexts39.
Thirdly, the remaining carbon budget is ‘zero sum’—meaning anyone’s excess share imposes on the share of others. While an approach to cutting emissions focused on efficiency gains may seem to be objective and politically attractive, this approach risks leading to the same level of emissions reduction for a lower cost—rather than the increased mitigation for the same cost, which equitable climate action within a finite carbon budget demands40,41. A fair share does not encroach on the share of others; the cost for the polluter is a relevant but secondary concern. The Paris Agreement is, ultimately, a commitment to cut emissions, not to cut emissions without any sacrifice. Since there are many ways of slicing up the carbon budget and no fixed rulebook on how to do it, there is an ever-present risk that self-declared ‘fair and ambitious’ pathways in fact represent neither42,43. Dedicated net-zero healthcare strategies can help ensure that ambitions and timelines are transparent and open to external scrutiny.
Such issues highlight the importance of pathways to net-zero healthcare that take full account of distributional concerns, historical responsibility and geographical context. This applies to efforts to integrate carbon emissions into the various healthcare resource allocation processes—be it in the evaluation of healthcare technologies44,45, procurement and commissioning46 or clinical service design47. From a priority-setting perspective, net-zero healthcare agendas must consider opportunity costs and how to manage trade-offs to protect health while cutting emissions39.
One option is to incorporate carbon emissions into existing healthcare resource allocation processes. This can, in theory, be achieved through placing a value on reductions in carbon emissions, which can be evaluated alongside other relevant outcomes. If two alternatives are similar in price and health outcomes then emissions can be a simple decision modifier—such as has been the case for the shift to lower carbon anesthetic agents44. Where there is a divergence between cost and health outcomes, this is less clear cut. Whether carbon emissions are incorporated into a multiple-criteria decision analysis (in order to rank alternatives) or directly monetized using a social cost of carbon (and incorporated into economic evaluations), the assigned weighting is contingent on value judgments. If the value assigned to reducing emissions is too low, it may have little impact on resource allocation48; if the value is too high, it risks sacrificing health.
Although directly incorporating emissions into the resource allocation process has the benefit of making trade-offs explicit within a specific set of decisions, it is more limited when considering healthcare’s carbon footprint as a whole, including supply chains, procurement, transport and estates. An alternative approach is to optimize health within a fixed ‘carbon budget’, thereby treating the goal of decarbonizing healthcare not in direct competition with health outcomes and financial budgets but as a distinct ethical concern29. The English National Health Service (NHS), for example, recommends a 10% minimum ‘net-zero and social value’ weighting to its procurement processes49 and has specific carbon reduction targets at the national and subnational levels50. Given the remaining global carbon budget is zero sum and emissions cause harm, the question of how to value reductions in emissions should take full account of both. We consider this in more depth through the case study of universal health coverage (UHC; Box 1).

Moving toward net-zero healthcare
As set out in the COP26 health program, the rapid development of low-carbon healthcare can help countries adapt to the effects of climate change and avoid being locked into carbon-intensive service delivery, which requires expensive retrofitting solutions later on. There are promising indications that decarbonizing healthcare can provide a rapid return on investment. The NHS in England has stated that the costs associated with cutting 80% of emissions can be recouped in three and a half years51. Aga Khan Health Services have described a 5-year return on investment for efforts to reduce their emissions from operations in Tanzania, Pakistan and Kenya by 60% (ref. 52). Further research to more fully quantify returns on investment, incorporate carbon emissions into healthcare resource allocation44,48 and better understand the barriers facing decision-makers at all levels of the healthcare system53,54 could all help accelerate the healthcare decarbonization agenda.
Aligning policy priorities to support investments in low-carbon healthcare remains especially important for health policymakers in low-income and middle-income countries, which often still have pervasive unmet basic healthcare needs and underdeveloped healthcare systems. For example, only 28% of health facilities in sub-Saharan Africa have reliable electricity, while, globally, health facilities serving a billion people have no electricity at all55. This not only increases dependence on inefficient, expensive and polluting generators, but also is associated with a range of negative health impacts56. At COP27, international agencies committed to electrifying 100,000 health facilities by 2030 which, although an important step, still represents a fraction of the 415,000 new health facilities that the WHO has estimated to be necessary for the delivery of the UHC agenda57. A ‘Green UHC’ must go beyond decarbonization to encompass climate resilience—preparing for, coping with and recovering from climate shocks. It must also include the profound environmental, societal and health consequences of climate change1. Further work to define a ‘Green UHC’ and integrate the sustainability and UHC agendas is urgently needed.
Since high-income countries have the most polluting healthcare systems and are responsible for most historical emissions and continue to be the highest emitters, they must take a lead in decarbonizing healthcare. Engagement of some of the major polluters in the COP26 Health Programme represents a crucial first step58,59. However, middle-income countries also have an increasingly important role in curbing healthcare’s carbon footprint globally. Given severely constrained healthcare budgets and less access to financial capital, decarbonizing healthcare in low-income and middle-income countries carries an opportunity cost, which should be taken into account. New national and international financial mechanisms at the climate–health interface that support the development of high-quality, low-carbon and climate-resilient health systems will be critical. Policymakers at all levels face hard choices in the years ahead—these must be met head on (Box 2).
Conclusion
The global movement to decarbonize healthcare presents new challenges and opportunities for health policymakers. While future temperature trajectories can be predicted with increasing certainty, how to fairly divide the dwindling carbon budget, both across countries and sectors, remains contingent on value judgments. A fair pathway to net-zero healthcare should be progressive, not flat; it should take population change and basic needs into account and ensure that the biggest polluters rapidly reach net zero in order to leave breathing room for others. Accelerating the net-zero healthcare agenda has the potential to not only reduce healthcare’s climate impact, but also inspire the societal transformation urgently needed to meet the Paris Agreement. In this crucial decade for climate action, the health sector must play its part.
References
Romanello, M. et al. The 2022 report of the Lancet Countdown on health and climate change: health at the mercy of fossil fuels. Lancet 400, 1619–1654 (2022).
Rogelj, J. D. et al. in Global Warming of 1.5 °C. An IPCC special report on the impacts of global warming of 1.5 °C above pre-industrial levels and related global greenhouse gas emission pathways, in the context of strengthening the global response to the threat of climate change, sustainable development, and efforts to eradicate poverty (eds. Masson-Delmotte, V. et al.) 93–174 (Cambridge Univ. Press, 2018).
COP26 Health Team. COP26 Health programme: Country commitments to build climate resilient and sustainable health systems. https://cdn.who.int/media/docs/default-source/climate-change/cop26-health-programme.pdf?sfvrsn=cde1b578_5 (2021).
World Health Organization. Alliance for action on climate change and health (ATACH). https://www.who.int/initiatives/alliance-for-transformative-action-on-climate-and-health (2022).
World Health Organization. COP26 health programme: country commitments. https://www.who.int/initiatives/alliance-for-transformative-action-on-climate-and-health/country-commitments (2022).
Pichler, P. P., Jaccard, I. S., Weisz, U. & Weisz, H. International comparison of health care carbon footprints. Environ. Res. Lett. 14, 064004 (2019).
Tennison, I. et al. Health care’s response to climate change: a carbon footprint assessment of the NHS in England. Lancet Planet Health 5, e84–e92 (2021).
Lenzen, M. et al. The environmental footprint of health care: a global assessment. Lancet Planet Health 4, e271–e279 (2020).
U.S. Department of Health & Human Services. HHS shares health sector emissions reduction and climate resilience announcements at COP27. https://www.hhs.gov/about/news/2022/11/10/hhs-shares-health-sector-emissions-reduction-climate-resilience-announcements-at-cop27.html (2022).
Eckelman, M. J. et al. Health care pollution and public health damage in the United States: an update. Health Aff. 39, 2071–2079 (2020).
Salas, R. N., Maibach, E., Pencheon, D., Watts, N. & Frumkin, H. A pathway to net zero emissions for healthcare. Br. Med. J. 371, m3785 (2020).
United Nations Environment Programme. Emissions gap report 2021. https://www.unep.org/resources/emissions-gap-report-2021 (2021).
O’Neill, D. W., Fanning, A. L., Lamb, W. F. & Steinberger, J. K. A good life for all within planetary boundaries. Nat. Sustain. 1, 88–95 (2018).
Chancel, L., Piketty, T., Saez, E., Zucman, G. World inequality report 2022. World Inequality Lab https://wir2022.wid.world/download/ (2022).
Millward-Hopkins, J. Inequality can double the energy required to secure universal decent living. Nat. Commun. 13, 5028 (2022).
Gazzotti, P. et al. Persistent inequality in economically optimal climate policies. Nat. Commun. 12, 3421 (2021).
Soergel, B. et al. Combining ambitious climate policies with efforts to eradicate poverty. Nat. Commun. 12, 2342 (2021).
IPSOS. Two-thirds of citizens around the world agree climate change is as serious a crisis as coronavirus. https://www.ipsos.com/en/two-thirds-citizens-around-world-agree-climate-change-serious-crisis-coronavirus (2020).
Holz, C., Kartha, S. & Athanasiou, T. Fairly sharing 1.5: national fair shares of a 1.5 °C-compliant global mitigation effort. Int. Environ. Agreem. Polit. Law Econ. 18, 117–134 (2018).
Hickel, J., O’Neill, D. W., Fanning, A. L. & Zoomkawala, H. National responsibility for ecological breakdown: a fair-shares assessment of resource use, 1970–2017. Lancet Planet. Health 6, e342–e349 (2022).
Robiou du Pont, Y. et al. Equitable mitigation to achieve the Paris Agreement goals. Nat. Clim. Change 7, 38–43 (2017).
Intergovernmental Panel on Climate Change. in Climate Change 2014: Mitigation of Climate Change. Contribution of Working Group III to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change Ch. 3 (Cambridge Univ. Press, 2014).
Matthews, H. D. et al. Opportunities and challenges in using remaining carbon budgets to guide climate policy. Nat. Geosci. 13, 769–779 (2020).
Robiou du Pont, Y. & Meinshausen, M. Warming assessment of the bottom-up Paris Agreement emissions pledges. Nat. Commun. 9, 4810 (2018).
Williges, K., Meyer, L. H., Steininger, K. W. & Kirchengast, G. Fairness critically conditions the carbon budget allocation across countries. Glob. Environ. Change 74, 102481 (2022).
Stone, C. D. Common but differentiated responsibilities in international law. Am. J. Int. Law 98, 276–301 (2004).
Young, I. M. Responsibility and global justice: a social connection Model. Soc. Philos. Policy 23, 102–130 (2006).
Gardiner, S. M. A perfect moral storm: climate change, intergenerational ethics and the problem of moral corruption. Environ. Values 15, 397–413 (2006).
Bhopal, A. & Bærøe, K. Dual duties to patient and planet: time to revisit the ethical foundations of healthcare? J. Med. Ethics https://jme.bmj.com/content/early/2022/12/21/jme-2022-108847 (2022).
Healthcare Without Harm. Global roadmap for health care decarbonization (Climate-smart health care series). https://healthcareclimateaction.org/roadmap (2021).
The World Bank. The World Bank in Middle Income Countries. https://www.worldbank.org/en/country/mic/overview (2022).
Bhopal, A., Bærøe, K. & Norheim, O. F. How do we decarbonise fairly? Emissions, inequities and the implications for net zero healthcare. J. R. Soc. Med. 115, 337–340 (2022).
Norheim, O. F. Ethical priority setting for universal health coverage: challenges in deciding upon fair distribution of health services. BMC Med. 14, 75 (2016).
G7 Health Ministers. G7 Health Ministers’ Communiqué, 20 May 2022, Berlin. https://www.g7germany.de/resource/blob/974430/2042058/5651daa321517b089cdccfaffd1e37a1/2022-05-20-g7-health-ministers-communique-data.pdf (2022).
Bressler, R. D. The mortality cost of carbon. Nat. Commun. 12, 4467 (2021).
Hubacek, K., Baiocchi, G., Feng, K. & Patwardhan, A. Poverty eradication in a carbon constrained world. Nat. Commun. 8, 912 (2017).
United Nations. Paris Agreement to the United Nations framework convention on climate change. Report no. T.I.A.S. no. 16-1104. https://unfccc.int/sites/default/files/resource/parisagreement_publication.pdf (2015).
Shue, H. Subsistence protection and mitigation ambition: necessities, economic and climatic. Br. J. Polit. Int. Relat. 21, 251–262 (2019).
Bhopal, A. & Norheim, O. F. Priority setting and net zero healthcare: how much health can a tonne of carbon buy? Br. Med. J. 375, e067199 (2021).
Sue-Chue-Lam, C., Shove, E. & Xie, E. The counterintuitive role of efficiency: implications for the ecological impact of health care. Lancet Planet. Health 6, e929–e930 (2022).
Shue, H. in Climate Ethics: Essential Readings 200–214 (Oxford Univ. Press, 2010).
Anderson, K., Broderick, J. F. & Stoddard, I. A factor of two: how the mitigation plans of ‘climate progressive’ nations fall far short of Paris-compliant pathways. Clim. Policy 20, 1290–1304 (2020).
Hickel, J. & Slamersak, A. Existing climate mitigation scenarios perpetuate colonial inequalities. Lancet Planet. Health 6, e628–e631 (2022).
McAlister, S., Morton, R. L. & Barratt, A. Incorporating carbon into health care: adding carbon emissions to health technology assessments. Lancet Planet. Health 6, e993–e999 (2022).
National Institute for Health and Care Excellence. NICE Strategy 2021 to 2026. https://static.nice.org.uk/NICE (2021).
NHS Supply Chain. Embedding Social Value in NHS Supply Chain 2022. https://www.supplychain.nhs.uk/news-article/embedding-social-value-in-nhs-supply-chain/ (2022).
Mortimer, F., Isherwood, J., Wilkinson, A. & Vaux, E. Sustainability in quality improvement: redefining value. Future Healthc. J. 5, 88–93 (2018).
de Preux, L. & Rizmie, D. Beyond financial efficiency to support environmental sustainability in economic evaluations. Future Healthc. J. 5, 103–107 (2018).
NHS England. Applying net zero and social value in the procurement of NHS goods and services (version 1). https://www.england.nhs.uk/greenernhs/publication/applying-net-zero-and-social-value-in-the-procurement-of-nhs-goods-and-services (2022).
Greener NHS. Delivering a ‘Net Zero’ National Health Service 2022. https://www.england.nhs.uk/greenernhs/publication/delivering-a-net-zero-national-health-service/ (2022).
Commonwealth Fund. Getting to net zero: one health system fights climate change 2022. https://www.commonwealthfund.org/publications/podcast/2022/jan/getting-to-net-zero-one-health-system-fights-climate-change (2022).
Aga Khan Development Network. Achieving net zero: how our health operations are slashing carbon emissions while saving thousands. https://the.akdn/en/resources-media/whats-new/our-stories/achieving-net-zero-how-our-health-operations-are-slashing-carbon-emissions-while-saving (2022).
Parker, J. Barriers to green inhaler prescribing: ethical issues in environmentally sustainable clinical practice. J. Med. Ethics https://jme.bmj.com/content/early/2022/08/17/jme-2022-108388 (2022).
Quitmann, C., Sauerborn, R., Danquah, I., Herrmann, A. ‘Climate change mitigation is a hot topic, but not when it comes to hospitals’: a qualitative study on hospital stakeholders’ perception and sense of responsibility for greenhouse gas emissions. J. Med. Ethics https://jme.bmj.com/content/early/2022/04/21/medethics-2021-107971 (2022).
World Health Organization. Energizing health: accelerating electricity access in health-care facilities. https://www.who.int/publications/i/item/energizing-health–accelerating-electricity-access-in-health-care-facilities (2023).
Mechtenberg, A. et al. Health care during electricity failure: the hidden costs. PLoS ONE http://www.ncbi.nlm.nih.gov/pmc/articles/PMC7641375/ (2020).
Stenberg, K. et al. Financing transformative health systems towards achievement of the health sustainable development goals: a model for projected resource needs in 67 low-income and middle-income countries. Lancet Glob. Health 5, e875–e887 (2017).
Dzau, V. J., Levine, R., Barrett, G. & Witty, A. Decarbonizing the US Health Sector—a call to action. N. Engl. J. Med. 385, 2117–2119 (2021).
Balbus, J. M., McCannon, C. J., Mataka, A. & Levine, R. L. After COP26—putting health and equity at the center of the climate movement. N. Engl. J. Med. 386, 1295–1297 (2022).
Hoegh-Guldberg, O. et al. in Global Warming of 1.5 °C: An IPCC Special Report on the impacts of global warming of 1.5°C above pre-industrial levels and related global greenhouse gas emission pathways, in the context of strengthening the global response to the threat of climate change, sustainable development, and efforts to eradicate poverty (eds. Masson-Delmotte, V. et al.) 175–312 (Cambridge Univ. Press, 2018).
Andrew, R. It’s getting harder and harder to limit ourselves to 2 °C. https://folk.universitetetioslo.no/roberan/t/global_mitigation_curves.shtml (2020).
Notre Dame Global Adaptation Initiative. Notre Dame Global Adaptation Initiative - Country Index. https://gain.nd.edu/our-work/country-index/rankings/ (2023).
United Nations. World Population Prospects 2019, volume I: Comprehensive Tables (ST/ESA/SER.A/426). Department of Economic and Social Affairs, Population Division. https://www.un.org/development/desa/pd/content/world-population-prospects-2019-volume-i-comprehensive-tables (2019).
Our World in Data. Population by world region, including UN projections. https://ourworldindata.org/grapher/world-population-by-region-with-projections (2023).
Rasheed, F. N. et al. Decarbonising healthcare in low and middle income countries: potential pathways to net zero emissions. Br. Med. J. 375, n1284 (2021).
World Health Organization. Primary health care on the road to universal health coverage: 2019 global monitoring report: executive summary. https://apps.who.int/iris/handle/10665/328913 (2019).
Jamison D. T. et al. Disease Control Priorities 3rd edn. (The World Bank: World Bank Publications, 2017).
Moses, M. W. et al. Funding and services needed to achieve universal health coverage: applications of global, regional, and national estimates of utilisation of outpatient visits and inpatient admissions from 1990 to 2016, and unit costs from 1995 to 2016. Lancet Public Health 4, e49–e73 (2019).
Author information
Authors and Affiliations
Contributions
Both authors contributed to the writing of this Perspective.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Medicine thanks Sonia Roschnik and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Primary Handling Editor: Karen O’Leary, in collaboration with the Nature Medicine team.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Bhopal, A., Norheim, O.F. Fair pathways to net-zero healthcare. Nat Med 29, 1078–1084 (2023). https://doi.org/10.1038/s41591-023-02351-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41591-023-02351-2
This article is cited by
-
Building healthy populations
Nature Medicine (2023)
