
Abstract
The Sustainable Development Goals include a target to reduce the global maternal mortality ratio (MMR) to less than 70 maternal deaths per 100,000 live births by 2030, with no individual country exceeding 140. However, on current trends the goals are unlikely to be met. We used the empirically calibrated Global Maternal Health microsimulation model, which simulates individual women in 200 countries and territories to evaluate the impact of different interventions and strategies from 2022 to 2030. Although individual interventions yielded fairly small reductions in maternal mortality, integrated strategies were more effective. A strategy to simultaneously increase facility births, improve the availability of clinical services and quality of care at facilities, and improve linkages to care would yield a projected global MMR of 72 (95% uncertainty interval (UI) = 58–87) in 2030. A comprehensive strategy adding family planning and community-based interventions would have an even larger impact, with a projected MMR of 58 (95% UI = 46–70). Although integrated strategies consisting of multiple interventions will probably be needed to achieve substantial reductions in maternal mortality, the relative priority of different interventions varies by setting. Our regional and country-level estimates can help guide priority setting in specific contexts to accelerate improvements in maternal health.
Similar content being viewed by others

Main
The Sustainable Development Goals (SDGs) set by the United Nations include a target to reduce the global maternal mortality ratio (MMR) to less than 70 maternal deaths per 100,000 live births by 2030, with no individual country exceeding 140 (ref. 1). While progress was made under the previous Millennium Development Goals, this area lags behind and the maternal mortality targets were not met2. Previous projections also found that although maternal deaths are projected to decline in the future, on current trends the projected decreases will fail to achieve the SDG maternal mortality target3,4. Although effective interventions exist to promote maternal health and address obstetric complications5, critical gaps in knowledge remain, especially around how these interventions may take place in various health systems in practice6. Monitoring progress and evaluating the effectiveness of strategies is further complicated by the lack of routine and complete information on maternal deaths from vital registration systems in many countries7, as well as underreporting and misclassification of maternal deaths, especially in early pregnancy and from complications of induced abortion and indirect obstetric causes8,9.
Statistical methods have been used by the United Nations3,10 and Institute for Health Metrics and Evaluation11,12 to estimate maternal health indicators based on the cross-sectional association between reported levels of maternal mortality and aggregate country-level factors, with per capita gross domestic product (GDP) being the largest driver of trends13. However, although these models can provide broad guidance to policymakers and offer insights into trends, the aggregate, cross-sectional nature of these models means that they are not suitable for exploring counterfactual scenarios to estimate the potential impact of realistic interventions. For example, although a cross-sectional association between GDP and maternal mortality may exist across countries, this does not imply that changes in GDP in a country over time would improve maternal health to a similar degree. Moreover, aggregate factors such as GDP do not offer actionable or realistic maternal health strategies for policymakers to consider.
Although economic growth can underpin progress, economic improvements alone are not sufficient, especially because the relationship between economic growth and health outcomes varies across countries, highlighting the need for more specific evidence on why some countries do better than others in preventing maternal deaths14. A previous analysis of success factors for reducing maternal and child mortality found that, although there is no standard formula, countries that have made substantial progress moved ahead in various areas, such as making progress across multiple sectors to address crucial health determinants and mobilizing partners across society using robust evidence for decision-making14. However, knowledge gaps remain in how to most successfully phase, scale and adapt such strategies for different countries.
Recommendations of specific interventions for countries to consider have been provided by the Disease Control Priorities project, a seven-year international collaborative effort to synthesize evidence and provide recommendations for health priorities in low- and middle-income countries (LMICs) for essential packages of interventions that provide good value for money and are feasible to implement15,16,17,18,19. Furthermore, analyses for the Lancet Commission on Investing in Health, which involved modeling scale-up of a range of such interventions in a set of LMICs to the existing rate in the ‘best-performing’ countries, found that countries could reach coverage levels of most interventions of at least 90% by 2035, yielding a large reduction in the average MMR of 74 countries, that is, from around 350 for the ‘low-coverage’ scenario to around 150 for the ‘high-coverage’ scenario20,21.
Updated analyses, however, estimated that maintaining the trends observed from 2010 to 2016 would not be sufficient to achieve convergence of coverage indicators for maternal mortality, with more aggressive scale-up of maternal health interventions needed, including structural investments in health systems, improvements in quality of care and use of robust evidence in a timely way for policy decisions and accountability22. While these analyses can provide broad guidance to policymakers, the use of a deterministic linear modeling approach23 means assumed relationships between coverage indicators and health outcomes may not hold in practice, and lack of accounting for parameter uncertainty, for example, intervention effect sizes, means that the results may not be robust to the large uncertainty surrounding maternal mortality indicators.
Previous efforts using a structural modeling approach and accounting for the ‘natural history’, that is, disease processes and outcomes in the absence of intervention, of maternal mortality have been undertaken, which examined the role of a comprehensive set of interventions, including health system linkages and family planning interventions, focused on specific countries such as India, Afghanistan, Nigeria and Mexico24,25,26,27. These analyses highlighted the importance of contextualizing the model to local situations and the impact of early intensive efforts to improve family planning and control of fertility choices, accompanied by a stepwise effort to scale up capacity for integrated maternal health services. However, these analyses did not provide global estimates.
To address these gaps, we developed a structural, individual-level model of global maternal health4, which can offer predictions of complex systems and, because it is based on a defined system of causal components and their relationships, allows realistic counterfactual scenarios to be evaluated28. This type of microsimulation modeling is increasingly recognized in epidemiology as another approach for causal inference because it uses the robust foundations of graphical causal models and can explore the effects of complex interventions that occur over prolonged periods of time29. In this study, we simulated various policy interventions aimed at improving maternal health, including individual interventions and integrated strategies consisting of multiple interventions. We provide estimates of their comparative impact, both globally and by region and country, to help guide decision-makers in different contexts seeking to accelerate improvements in maternal health. Table 1 summarizes our findings and policy implications.
Results
Interventions and strategies
We compared the effectiveness of various policies to reduce maternal mortality, ranging from individual interventions to integrated strategies. Following previously used typologies for maternal health interventions16,17,18,19,24, we categorized policies as family planning interventions, for example, contraception, medical abortion; community-based interventions, for example, antenatal care (ANC), skilled birth attendants (SBAs) for home births; facility-based interventions, for example, facility births, availability of clinical services; and system-relevant interventions, for example, linkages to care and quality of care (Table 2). We also modeled combinations of individual interventions to evaluate the impact of integrated strategies (Table 3).
Global maternal mortality
We found that individual interventions yielded fairly small reductions in maternal mortality, with the largest individual impact coming from increasing the number of women who deliver at facilities (projected global MMR in 2030 of 111, 95% UI = 94–129), followed by improving the quality of care at facilities (projected global MMR of 140, 95% UI = 113–159) (Table 4). However, the potential gains from other individual policy interventions were relatively modest.
Instead, integrated strategies that include multiple interventions will probably be needed to substantially accelerate improvements in maternal mortality. Globally, we found that increasing facility births, improving the availability of clinical services at facilities and improving linkages to care (for example, recognition of complications and appropriate referrals and transportation) would yield large improvements, with a projected global MMR of 104 (95% UI = 87–121) in 2030 (Table 4). However, we found that even with this set of interventions, the global SDG target would not be met if improvements in quality of care are neglected. Instead, we found that efforts to improve quality of care in addition to facility-based and linkage interventions will be necessary to potentially achieve the SDG target, yielding a projected global MMR of 72 (95% UI = 58–87) in 2030, with large improvements in LMICs (Table 4).
Family planning interventions also offer the potential for meaningful improvements and can reduce deaths from abortion-related mortality and indirect causes (via reduced pregnancy exposure), which are largely unaffected by the other policy interventions that we modeled (Table 5). Although all strategies reduced the total number of maternal deaths compared to our baseline scenario of current trends, we found small relative increases for particular causes of death in some scenarios (Table 5). This finding reflects the fact that as more women survive pregnancy and labor, the number of deaths from subsequent risks may increase despite reductions in overall mortality, highlighting the need for a comprehensive view of maternal mortality that considers competing risks. For example, increasing the proportion of women who give birth in medical facilities is estimated to reduce total maternal deaths by nearly 30% but may lead to small increases in late and indirect maternal deaths as more women survive direct maternal complications and face these other risks (Table 5).
Although we found that an integrated strategy including facility-based and system-relevant interventions (Table 3) could potentially achieve the SDG target in reducing maternal mortality, there is uncertainty around whether the goal could be achieved by 2030 (Fig. 1). Instead, due to the multifactorial nature and many causes of maternal death, a comprehensive integrated strategy including community-based and family planning interventions will probably be needed to achieve the global SDG target by 2030, with a projected global MMR of 58 (95% UI = 46–70).

The lines indicate the means, the shaded regions indicate the 95% UIs and the dashed line indicates the SDG target 3.1 of a global MMR of 70 by 2030.
Region-specific impacts
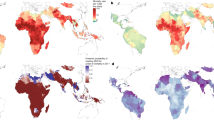
Overall, the projected impact of various strategies and comprehensive scale-up varied both across and within continents, depending on the baseline situation in each location, with high-income regions such as Europe and North America projected to have smaller reductions in maternal mortality due to better status quo indicators, while other regions would experience large benefits from a comprehensive scale-up, especially in Africa and Asia (Extended Data Fig. 1).
Because the profile of causes of maternal death varies according to location4, the relative impact of different strategies also varies according to region (Extended Data Fig. 2), highlighting the need to consider the local context when designing and implementing policies. For example, family planning could have a large impact in areas of Asia and sub-Saharan Africa where fertility is still high. Even within regions there are differences in priority setting according to country. For example, in Southern Asia, family planning interventions are projected to have the largest impact among (noncomprehensive) integrated strategies in Afghanistan, where fertility is high. In contrast, in countries such as India, which have already experienced substantial declines in fertility, the incremental benefits of family planning alone are small, with far greater reductions in maternal mortality achieved by integrated strategies that focus on linkages to facilities and improved quality of care. Results for each modeled country and territory are available in the Appendix 1.
Discussion
We found that an integrated strategy, including facility-based and system-relevant interventions, could substantially improve maternal health but it is unlikely to achieve the SDG global maternal mortality target by 2030 without also including community-based and family planning interventions as part of a comprehensive strategy. Among the interventions in such a strategy, we found that increasing the proportion of births that occur at health facilities is the single intervention with the largest impact on maternal mortality. However, while increasing facility delivery and linkages to care for complications from the community are necessary to substantially improve maternal health, these policies alone may not be sufficient if quality of care is not also improved.
This finding echoes previous evaluations of real-world interventions. For example, Janani Suraksha Yojana, a conditional cash-transfer program to incentivize facility delivery in India, succeeded in substantially increasing facility births but had no significant effect on mortality due to lack of focus on the quality of facilities30,31. Similarly, the Better Birth trial succeed in improving the adherence of SBAs to essential birth practices but had no significant impact on health outcomes32. These findings highlight the necessity of considering other contextual factors related to health system quality.
The complex interdependencies of service delivery mean that a narrow focus on one aspect of the care continuum is unlikely to substantially improve outcomes. Identifying and estimating the relative contribution of these factors in a structural model can help inform policymakers on the likely impact of such interventions before they are implemented, including the impact of competing risks for other health outcomes.
At the global level, these results can reveal general insights that can be broadly applied, such as that individual policies generally offer modest incremental gains and are less effective than integrated strategies, especially those that include enhanced linkages to care along the referral pathway, for example, recognition and referral, and timely transport to health facilities. These insights echo previous findings and our general estimates are similar to previous model-based studies. For example, a previous study that focused on India estimated that integrated efforts to improve family planning, access to safe abortion and scale up high-quality maternal health services could reduce direct maternal deaths by more than 75%24. The Guttmacher Institute Adding It Up report estimated that if all women had access to modern contraceptives and all pregnant women received quality care, maternal deaths would drop by 62% in LMICs33, which is very similar to our comprehensive strategy that yields a 60.1% (95% UI = 54.9–65.0%) decrease globally. The report also estimated that meeting all needs for pregnancy-related care, with no change in levels of contraceptive care, would yield a 50% reduction in maternal deaths in LMICs33, which is similar to our strategy including facility-based, system-relevant and quality-of-care interventions that yields an estimated 51.0% (95% UI = 45.1%–56.1%) global reduction. These findings are also similar to a previous analysis using the LiST model, which estimated that 51% of maternal deaths could be averted in 75 high-burden countries by achieving high coverage of ANC and care during labor and childbirth34.
Our model findings also align with real-world evidence, such as a program in Dar es Salaam, Tanzania that implemented multiple evidence-based health system strengthening interventions addressing the continuum of care and yielded a sixfold improvement in quality of care and a 47% reduction in maternal mortality35. Such programs show that implementing integrated strategies and achieving substantial reductions in maternal mortality can be feasible even in resource-constrained settings.
Although our general findings are similar to previous estimates, a high-level global view can also obscure differences and may not provide adequate guidance for policymakers in different contexts. Instead, our regional and country-specific estimates of the impact of various policies are probably more informative for decision-making. These results also highlight the importance of considering a dashboard of multiple indicators when setting targets and assessing progress (in addition to MMR), which reflect differences in baseline indicators and health system priorities that vary according to context. For example, family planning interventions that lower exposure to pregnancy but have smaller effects on obstetrical risk may have larger impacts on indicators such as lifetime risk (LTR) of maternal death and total maternal deaths, while having a smaller impact on MMR. Multiple indicators are therefore needed to monitor progress both globally and especially at the country-level where local contexts may vary substantially. Our country-level comparative effectiveness estimates can help provide guidance on which types of policies local decision-makers should prioritize as interventions are scaled up.
Although we provide estimates of such policy impacts for 200 countries and territories, the lack of data for many variables of interest for some locations, such as the distribution of emergency obstetric care (EmOC) facility types where women give birth, mean that we had to make certain assumptions when developing the model. We used a hierarchical modeling approach to regularize estimates that were available and impute parameter values for countries and territories for which we had no data4. We account for uncertainty around all model parameters and report uncertainty intervals for all model outcomes but recognize that as these are conditional on the model structure, there are probably other sources of uncertainty, for example, structural assumptions, which are not reflected in our reported measures of uncertainty. For our projections, we also assumed that current trends will continue (for each model parameter that incorporates secular trends) for our baseline comparator strategy. Although our estimates can provide insight into the comparative effectiveness of policies to improve maternal health, we recognize the need for decision-makers to also consider the costs of implementing such policies. Indeed, in previous work we identified more and less efficient ways of scaling up interventions in India25. Although we do not currently include costs in the Global Maternal Health (GMatH) model, an advantage of our approach is that we can assess the construction of such strategies in more realistic, nuanced ways; in future research, we plan to extend our approach to consider costs.
Examining the cost-effectiveness and budget impact of interventions was outside the scope of this study but such analyses can also provide information regarding the feasibility of different policies. We set minimum coverage targets for this analysis informed by the mean levels of high-income countries, instead of modeling convergence with the best-performing countries, to help address concerns regarding feasibility. However, substantial investments will still probably be required to achieve these targets. This point is especially important because we modeled the incremental impact of intervention scale-up in addition to baseline trends, which we assume will continue, but which cannot be taken for granted because progress to date has been due to sustained efforts over long periods of time, which will not only have to be continued but expanded on.
This study has several limitations. Even under comprehensive scale-up, we found that there would still exist large differences in maternal mortality between low-income and high-income countries. This is probably due to the role of indirect maternal deaths, which are heterogeneous across countries and which we assumed were unaffected by our modeled clinical and health system interventions. We also assumed that trends in demographic composition, typically a lower education level and rural location in low-income countries, would continue on projected trends and not be affected by policy interventions. Our assumption of lack of direct impact on late and indirect maternal deaths of the modeled policies means that our estimates may be conservative. Additional interventions to improve women’s education and address indirect causes of maternal death, for example, malaria and HIV, are therefore probably needed in addition to interventions that address direct causes of maternal deaths.
Despite these limitations, we find that our structural modeling approach has high predictive accuracy4; because it models the underlying causal relationships between factors that impact various aspects of maternal health, it allows for more realistic counterfactual estimates to be made. In addition to insights from our global estimates, we find that the relative priority of specific interventions varies according to region. Our regional and country-level comparative effectiveness estimates can therefore help guide planning and priority setting in various contexts to accelerate improvements in maternal health.
Methods
Simulation model overview
We developed the GMatH microsimulation model (previously described elsewhere)4 to simulate the reproductive histories of individual women in 200 countries and territories, accounting for heterogeneity in education and urban or rural location, family planning preferences and history of maternal complications (see http://gmath-model.org/ for online model documentation). The model progresses in monthly cycles and follows an open population, that is, with new female infants entering each cycle, allowing population-level indicators to be estimated by calendar year. The model simulates pregnancy based on age, breastfeeding status and contraceptive use, which is informed by women’s individual fertility preferences and whether their need for contraception is met. Pregnant women may experience ectopic pregnancy or miscarriage, and unintended pregnancies also face a risk of induced abortion, a proportion of which may be ‘unsafe’ (for example, when conducted by untrained personnel) and associated with higher morbidity and mortality. Complications associated with pregnancy and childbirth are modeled based on individual-level risk factors, for example, anemia, with incidence and case fatality rates impacted by various health system factors, such as ANC visits, appropriate referral and transportation to facilities (which we assume are implicitly impacted by factors such as cost of care), availability of specific clinical interventions, level of care available and quality of care.
We included a parameter for ‘quality of care’ to account for health system-level and facility-level factors not explicitly included in the model. Quality of care has been defined as the ‘degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge’36. Although it is a broad concept, the Institute of Medicine has described quality of care as having six key features: care that is safe; effective; patient-centered; efficient; timely; and equitable. Although all these features are important, there are often particularly substantial deficiencies regarding patient safety, for example, iatrogenic harm; effectiveness, for example, providers may fail to provide the appropriate treatment even if it is available; and patient-centeredness, for example, patients may opt out of or not adhere to treatment if they lack confidence in the health system31. We therefore included this parameter in the model to account for residual differences in maternal mortality not explained by differences in the incidence or severity of obstetric complications and availability or efficacy of clinical interventions, such as improved professionalization of health workers. Thus, this parameter is focused on the quality of clinical care received at health facilities after accounting for other factors both within and outside the health system.
In addition to death from pregnancy-related complications, that is, direct maternal deaths, women also face risks of indirect maternal deaths and age-specific competing mortality from other causes.
The model was calibrated to empirical data on a range of maternal health-related indicators, accounting for underreporting of maternal deaths, and had high predictive accuracy for a test set of external data not used to fit the model, with coverage probabilities, that is, the proportion of times the empirical point estimate fell within the model’s 95% UI of 96.0% for maternal mortality indicators and a mean error of 2.6 deaths (s.e. = 8.9) for total maternal deaths4.
Interventions and strategies
Using the model, we compared the effectiveness of a range of different policies to reduce maternal mortality, ranging from individual interventions to integrated strategies. We compared the impact of each policy to a baseline scenario of current trends, that is, no new intervention of scale-up but with current trends due to previous and existing efforts assumed to continue, and modeled the implementation of each policy by scaling up the relevant parameters between 2022 and 2030 to achieve minimum coverage targets informed by the mean level of high-income countries in 2022, assuming a linear scale-up over time. Following previously used typologies for maternal health interventions16,17,18,19,24, we categorized interventions as family planning, community-based, facility-based and system-relevant interventions (Table 2).
Family planning interventions include reducing unmet need for contraception and reducing the proportion of induced abortions that are unsafe, allowing women more control to achieve their fertility preferences, which we assume are unaffected by these interventions. Community-based interventions include increased ANC visits to improve health status during pregnancy, for example, anemia, and improve recognition of complication danger signs, as well as increased coverage of home births attended by an SBA, who can provide basic interventions and refer complications to facilities for emergency care.
Facility-based interventions include increasing the number of women who give birth in a health facility (regardless of facility type), and improving the availability of clinical services at facilities. Three levels of facilities were modeled based on the level of EmOC they are supposed to be able to provide, based on World Health Organization guidelines: non-EmOC (no EmOC) facility; BEmOC facility; and CEmOC facility37. The delivery site for each woman was modeled based on urban or rural location and educational level, thus accounting for differential EmOC access both across and within countries. Although facilities that are designated as CEmOC are theoretically supposed to provide all required obstetric clinical services, for example, surgery, in practice facilities may only offer a subset of services that they would normally be expected to provide due to equipment, drug and personnel shortages, as well as broader infrastructure factors, such as lack of stable power supply38,39. Therefore, the GMatH model simulates the availability of specific clinical services at each facility type within each country, assuming that although CEmOC facilities in a given context may not offer all necessary services, the availability of services is higher than at BEmOC or non-EmOC facilities in the same context4.
As a conservative assumption, we assumed that increasing EmOC services alone has no clinical impact on late maternal deaths or indirect maternal deaths, for example, malaria or HIV-related deaths exacerbated by pregnancy, as these would probably require other targeted, that is, non-obstetric interventions, or on other direct maternal deaths, which are treated mainly with supportive care that we assumed could be impacted by improving quality of care.
System-relevant policies include improving the quality of care at facilities and improving linkages to care along the referral pathway, such as recognition and referral of complications, timely transportation and transfers to facilities with the appropriate level of care to manage the complication at hand. We also modeled combinations of these individual policies to evaluate the impact of integrated policy strategies (Table 3).
Statistical analysis
We compared the impact of the policy interventions on projected maternal indicators, including total maternal deaths, MMR and LTR of maternal deaths. We simulated 1,000 iterations of each policy, sampling from the 100 best-fitting parameter sets in each iteration to account for both first-order, that is, individual-level, stochastic, and second-order, that is, parameter uncertainty. For all model outcomes, we report the mean and 95% UIs, calculated as the 2.5 and 97.5 percentiles of the simulation results. The GMatH model was developed in Java v1.8.0.
Ethics and inclusion statement
All data for this study, including from LMICs, were obtained from publicly available sources. One colleague (B.S.D.) is from an LMIC and the corresponding author (Z.J.W.) is originally from an LMIC and is now based in a high-income country. We fully endorse the Nature Portfolio guidance on LMIC authorship and inclusion. Because this work builds on previous modeling work, authorship was based, in part, on previous participation and collaboration. However, we are strongly committed to collaboration with researchers from LMICs in future work, especially for analyses focused on specific contexts or countries.
This research is locally relevant to all countries included as we report findings by country, providing local policymakers with important data on the impact of maternal health interventions.
Because our modeling approach used only publicly available data and published data from the medical literature for each country, ethics review was not required. The data collection and analysis techniques used raised no risks pertaining to stigmatization, incrimination, discrimination, animal welfare, the environment, health, safety, security or other personal risks. No biological materials, cultural artifacts or associated traditional knowledge has been transferred out of any country. In preparing the manuscript, the authors reviewed relevant studies from all countries for which data were available.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The simulation results are available in a public data repository at https://doi.org/10.7910/DVN/4F56ZB. We have also provided documentation for all model parameters, including data sources, assumptions and model implementation details online (http://gmath-model.org/).
Code availability
No software was used for any primary data collection in this study. The GMatH simulation model was developed in Java v.1.8.0 and statistical analyses were performed in R v.3.6.1. The pseudocode describing the simulation algorithm is available at http://gmath-model.org/1_7_Pseudocode.html. Requests for more code details should be addressed to Z.J.W.
References
EPMM working group. Strategies Toward Ending Preventable Maternal Mortality (EPMM) (World Health Organization, 2015).
United Nations. The Millennium Development Goals Report 2015 (United Nations, 2015).
WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. Trends in Maternal Mortality 2000 to 2017 (World Health Organization, 2019).
Ward, Z. J., Atun, R., King, G., Sequeira Dmello, B. & Goldie, S. J. Simulation-based estimates and projections of global, regional, and country-level maternal mortality by cause, 1990–2050. Nat. Med. (in the press).
The Partnership for Maternal, Newborn & Child Health. Essential Interventions, Commodities and Guidelines for Reproductive, Maternal, Newborn and Child Health (World Health Organization, 2011).
Kendall, T. & Langer, A. Critical maternal health knowledge gaps in low- and middle-income countries for the post-2015 era. Reprod. Health 12, 55 (2015).
Say, L. et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob. Health 2, e323–e333 (2014).
Graham, W. J. Now or never: the case for measuring maternal mortality. Lancet 359, 701–704 (2002).
Main, E. K. Maternal mortality: new strategies for measurement and prevention. Curr. Opin. Obstet. Gynecol. 22, 511–516 (2010).
Alkema, L. et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Maternal Mortality Estimation Inter-Agency Group. Lancet 387, 462–474 (2016).
Kassebaum, N. J. et al. Global, regional, and national levels and causes of maternal mortality during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 384, 980–1004 (2014).
Kassebaum, N. H. et al. Global, regional, and national levels of maternal mortality, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 388, 1775–1812 (2016).
Abouzahr, C. New estimates of maternal mortality and how to interpret them: choice or confusion? Reprod. Health Matters 19, 117–128 (2011).
Kuruvilla, S. et al. Success factors for reducing maternal and child mortality. Bull. World Health Organ. 92, 533–544 (2014).
Jamison, D. T. et al. Universal health coverage and intersectoral action for health: key messages from Disease Control Priorities, 3rd edition. Lancet 391, 1108–1120 (2018).
Stover, J., Hardee, K., Ganatra, B., García Moreno, C. & Horton, S. in Reproductive, Maternal, Newborn, and Child Health: Disease Control Priorities 3rd edn, Vol. 2 (eds Black R. E. et al.) Ch. 6 (The International Bank for Reconstruction and Development and The World Bank, 2016).
Gülmezoglu, A. M. et al. in Reproductive, Maternal, Newborn, and Child Health: Disease Control Priorities 3rd edn, Vol. 2 (eds Black, R. E. et al.) Ch. 7 (The International Bank for Reconstruction and Development and The World Bank, 2016).
Lassi, Z. S., Kumar, R. & Bhutta, Z. A. in Reproductive, Maternal, Newborn, and Child Health: Disease Control Priorities 3rd edn, Vol. 2 (eds Black, R. E. et al.) Ch. 14 (The International Bank for Reconstruction and Development and The World Bank, 2016).
Bollinger, L. A. & Kruk, M. E. in Reproductive, Maternal, Newborn, and Child Health: Disease Control Priorities 3rd edn, Vol. 2 (eds Black, R. E. et al.) Ch. 15 (The International Bank for Reconstruction and Development and The World Bank, 2016).
Jamison, D. T. et al. Global health 2035: a world converging within a generation. Lancet 382, 1898–1955 (2013).
Stenberg, K. et al. Advancing social and economic development by investing in women’s and children’s health: a new Global Investment Framework. Lancet 383, 1333–1354 (2014).
Watkins, D. A. et al. Alma-Ata at 40 years: reflections from the Lancet Commission on Investing in Health. Lancet 392, 1434–1460 (2018).
Walker, N., Tam, Y. & Friberg, I. K. Overview of the Lives Saved Tool (LiST). BMC Public Health 13, S1 (2013).
Goldie, S. J., Sweet, S., Carvalho, N., Natchu, U. C. & Hu, D. Alternative strategies to reduce maternal mortality in India: a cost-effectiveness analysis. PLoS Med. 7, e1000264 (2010).
Hu, D., Bertozzi, S. M., Gakidou, E., Sweet, S. & Goldie, S. J. The costs, benefits, and cost-effectiveness of interventions to reduce maternal morbidity and mortality in Mexico. PLoS ONE 2, e750 (2007).
Erim, D. O., Resch, S. C. & Goldie, S. J. Assessing health and economic outcomes of interventions to reduce pregnancy-related mortality in Nigeria. BMC Public Health 12, 786 (2012).
Carvalho, N., Salehi, A. S. & Goldie, S. J. National and sub-national analysis of the health benefits and cost-effectiveness of strategies to reduce maternal mortality in Afghanistan. Health Policy Plan 28, 62–74 (2013).
Murray, C. J., Ezzati, M., Lopez, A. D., Rodgers, A. & Vander Hoorn, S. Comparative quantification of health risks conceptual framework and methodological issues. Popul. Health Metr. 1, 1 (2003).
Arnold, K. F., Harrison, W. J., Heppenstall, A. J. & Gilthorpe, M. S. DAG-informed regression modelling, agent-based modelling and microsimulation modelling: a critical comparison of methods for causal inference. Int. J. Epidemiol. 48, 243–253 (2019).
Randive, B., Diwan, V. & De Costa, A. India’s conditional cash transfer program (the JSY) to promote institutional birth: is there an association between institutional birth proportion and maternal mortality? PLoS ONE 8, e67452 (2013).
Scott, K. W. & Jha, A. K. Putting quality on the global health agenda. N. Engl. J. Med. 371, 3–5 (2014).
Semrau, K. E. A. et al. Outcomes of a coaching-based WHO Safe Childbirth Checklist program in India. N. Engl. J. Med. 377, 2313–2324 (2017).
Sully, E. A. et al. Adding It Up: Investing in Sexual and Reproductive Health 2019 (Guttmacher Institute, 2020).
Bhutta, Z. A. et al. Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost? Lancet 384, 347–370 (2014).
Sequeira Dmello, B. et al. Learning from changes concurrent with implementing a complex and dynamic intervention to improve urban maternal and perinatal health in Dar es Salaam, Tanzania, 2011–2019. BMJ Glob. Health 6, e004022 (2021).
Institute of Medicine. Medicare: a Strategy for Quality Assurance (National Academy Press, 1990).
WHO, UNFPA, UNICEF, AMDD. Monitoring Emergency Obstetric Care: a Handbook (World Health Organization, 2009).
Bailey, P., Paxton, A., Lobis, S. & Fry, D. The availability of life-saving obstetric services in developing countries: an in-depth look at the signal functions for emergency obstetric care. Int. J. Gynecol. Obstet. 93, 285–291 (2006).
Mbonye, A. K. & Asimwe, J. B. Factors associated with skilled attendance at delivery in Uganda: results from a national health facility survey. Int. J. Adolesc. Med. Health 22, 249–255 (2010).
Acknowledgements
Z.J.W. and S.J.G. received support from the John D. and Catherine T. MacArthur Foundation (grant no. 10-97002-000-INP). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
Z.J.W. acquired the data, performed the analyses and developed the model based on a conceptual framework developed by S.J.G. R.A., G.K. and B.S.D. provided critical feedback on the modeling approach and assumptions. All authors interpreted the results, contributed to the writing of the article and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Medicine thanks Patrick Gerland, Akira Shibanuma and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Primary Handling Editor: Ming Yang, in collaboration with the Nature Medicine team.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
Extended Data Fig. 1 Projected MMR by geographic area and integrated strategy.
Lines indicate means. Shaded regions indicate 95% UIs. Dashed line indicates SDG target 3.1 of a global MMR of 70 by 2030.
Extended Data Fig. 2 Projected Reduction in Maternal Deaths 2030–2050 by Region and Integrated Strategy.
Reduction is mean percent reduction in projected maternal deaths in 2030–2050 (cumulative) compared to Baseline projections. Horizontal lines indicate 95% uncertainty intervals, calculated as the 2.5 and 97.5 percentiles of the simulation results.
Supplementary information
Supplementary Information
Supplementary Appendix 1 (country results).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ward, Z.J., Atun, R., King, G. et al. A simulation-based comparative effectiveness analysis of policies to improve global maternal health outcomes. Nat Med 29, 1262–1272 (2023). https://doi.org/10.1038/s41591-023-02311-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41591-023-02311-w
